






A 70-year-old patient was referred for multi-slice computed tomography (MSCT) of the coronary arteries due to anginal symptoms over the past 3 months. The patient’s comorbidities included atrial fibrillation and diabetes mellitus.
An electrocardiography-triggered MSCT of the coronary arteries was performed using a 128-slice Somatom Flash Dual Source Siemens device. MSCT of the coronary arteries did not reveal significant lesions. However, the multiplanar reconstruction and 3D images revealed the anterior interventricular vein (AIV) running parallel to the left anterior descending artery (LAD) in the interventricular sulcus. The AIV is in close contact with the left main (LM) coronary artery at the bifurcation into the LAD and left circumflex arteries, and it drains into the left atrium (LA) on the anteromedial wall (Figures 1 A, B). The remaining venous system shows normal anatomical configuration, with the coronary sinus draining into the right atrium at the expected position, along with the presence of the semicircular Thebesian valve at the same level as the Eustachian valve. Following the MSCT of the heart, a transesophageal echocardiographic examination (TEE) was conducted, which revealed the drainge point of the AIV into the LA (Figure 1 C). Furthermore, color Doppler confirmed the flow through the AIV (Figure 1 D).
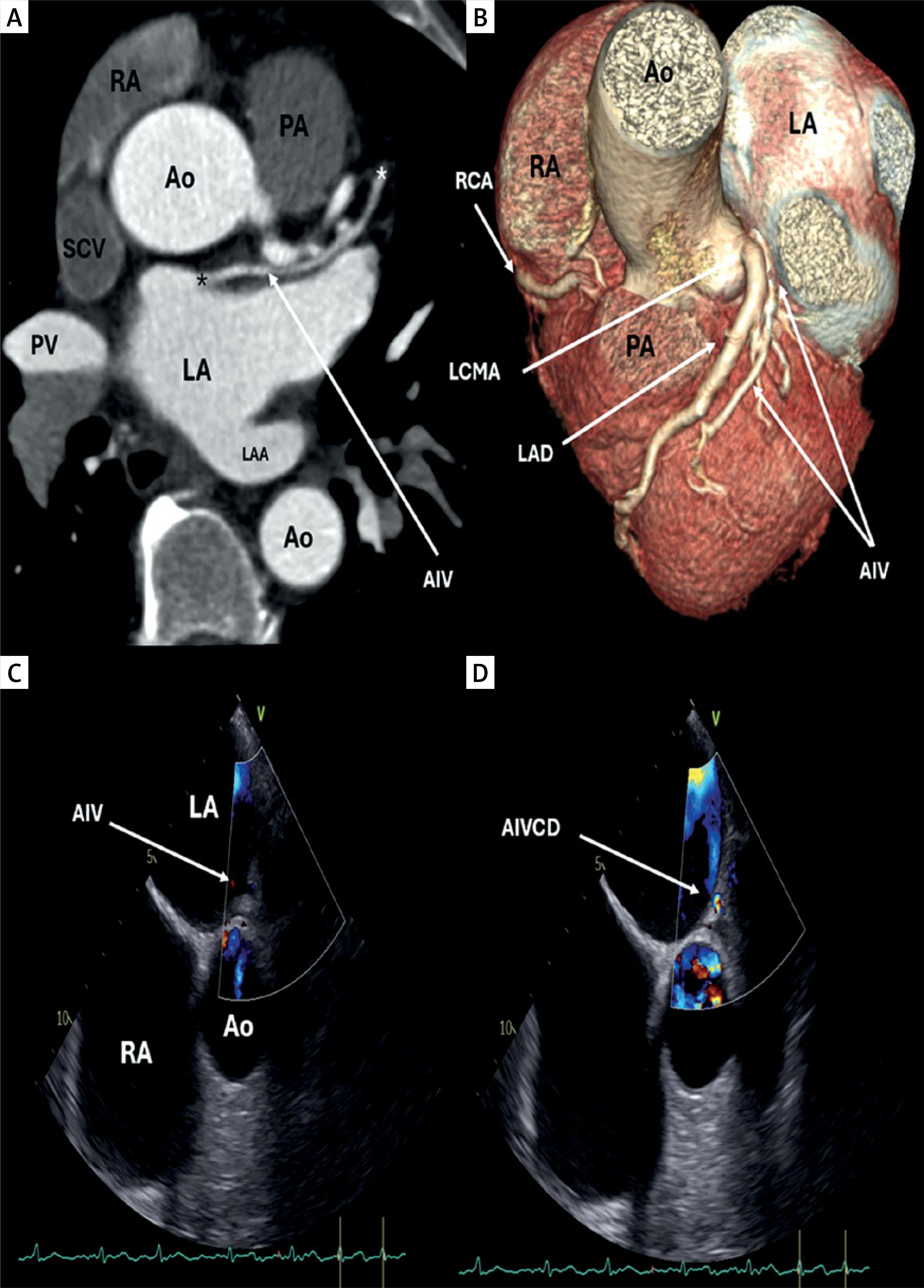
Figure 1
A – Multi-slice computed tomography (MSCT) axial 2D reconstruction of the left atrium (LA), showing the anterior interventricular vein (AIV) originating from the left ventricle (LV) (white asterisk), draining into the LA (black asterisk); B – MSCT 3D reconstruction showing the relation between the left anterior descending artery (LAD), left main coronary artery (LMCA), and AIV. C – Transesophageal echocardiography showing drainage point of the AIV into the LA. D – Color Doppler confirming flow through the AIV
RA – right atrium, Ao – aorta, PA – pulmonary artery, SCV – superior vena cava, PV – pulmonary vein, LAA – left atrial appendage, AIVCD – anterior interventricular vein color Doppler.
MSCT with prospective electrocardiography-gating seems to be a perfect tool for diagnostic imaging of coronary vessels in patients in all age groups [1]. MSCT of the coronary veins is gaining increasing importance in cardiology, as detailed mapping of the coronary veins is essential for certain procedures such as implantable cardioverter-defibrillator placement, pacemaker implantation, and ablation for arrhythmias to ensure patient safety [2]. The AIV usually originates from the lower or middle third of the anterior interventricular groove. It ascends parallel to the left anterior descending coronary artery and then turns posteriorly at the atrioventricular groove and terminates at the great cardiac vein [3]. Abnormalities in drainage of the great cardiac vein are interesting due to its rarity and likely to be underreported, with most cases found incidentally in cardiac imaging and autopsy studies [4]. AIV drainage into the left atrium is extremely rare. Sakrana et al., in their presentation of 2 cases, stated that only 3 cases with the same anomaly had been described [2]. The curiosity of our case is that this anomaly is not combined with persistent superior vena cava, which is usually the case when AIV drainage into the LA is found.