








Introduction
Sitting, as a daily working posture and a way of spending leisure time, constitutes approximately 50-60% of the average adult’s daily routine [1]. In the present era, administrative professionals spend up to 82% of their working hours in a seated position [2,3]. Initially, the emphasis on reducing the consequences of prolonged sitting during working hours was primarily due to its impact on the cardiovascular system and the prevalence of obesity. According to a systematic review [4], health guidelines for the general population focus on reducing overall sitting time throughout the day, whether at work or during leisure. However, beyond other systems, prolonged sitting is deemed hazardous to the musculoskeletal system [5], being a source of discomfort or pain. This is explained by hypotheses suggesting that the cause lies in factors such as low activity levels and a predominance of passive structure loading [6]; postural changes, such as flattening or accentuation of spinal curvatures over the sitting interval [7]; chronic deconditioning associated with habitually lower activity levels, leading to fatigue and the potential occurrence of repetitive strain injuries [6].
Further studies comparing seated work with sit-stand desks found higher self-reported fatigue, feelings of low energy during sitting, as well as reduced concentration and productivity [8,9]. Verticalization has positive effects on other systems beyond the musculoskeletal system, as indicated by a study [1], whose authors argue that replacing sedentary behavior with standing or low-level physical activity can reduce the risk of lifestyle-related diseases and mortality without achieving a level of moderate to vigorous physical activity (MVPA). Musculoskeletal pain is highly prevalent among computer users, encompassing neck and shoulder pain, as well as pain in the arms and wrists, with a prevalence ranging from 20.3% to 56.1% [10]. Musculoskeletal discomfort associated with computer work manifests through physical strain, psychosocial stress, total time spent working with computers, workstation setup, and organizational factors [11].
In clinical practice, pain is the most common reason for seeking professional help [12]. Unfortunately, pain, as such, may only appear in response to the decompensation of chronic conditions, such as long-term soft tissue degeneration (also known as Repetitive Strain Injury), where one’s morphology changes over prolonged irritation, leading to fibrosis, atrophy, or infiltration by fat cells [12,13]. Lateral epicondylitis, a diagnosis associated with tendinopathy of the wrist and hand extensor group, is most linked to hypertonia of the extensor carpi radialis brevis and degeneration of its insertion, among other extensors. Given its frequent occurrence in a group with a repetitive job nature and emphasis on precision, administrative workers may precisely constitute this set. There is a significant correlation between work style, lack of breaks, pain, and loss of productivity. All of these factors can, in turn, affect the individual and their environment and subsequently put them in a ‘spiral’ which is compounded by ill health which reduces their productivity, this in turn increases pressure on the psyche, for example, which compounds their current painful state [14].
Although pain should have a signaling character, as suggested by its definition, unfortunately, in the case of prolonged exposure of the organism to nociceptive stimuli or dysfunctional neuromuscular adaptation in response to a stimulus, disability may develop, transitioning into chronicity. Physiotherapy is commonly prescribed in response to these situations, as well as for the prevention of painful conditions (global physical activity, individually targeted exercise programs, training of specific motor skills, and functional tasks). Understanding the origin of nociceptive sensations and targeting therapy and prevention correctly can help restore or prevent subsequent long-term complications and financial expenditures [12].
Despite differing opinions regarding ergonomics and its practical application, a study by Hoe et al. [15] suggests that computer ergonomics training should involve educating the target group about identifying risk factors, selecting and using appropriate work procedures, equipment, and individual settings that meet individual needs. According to a systematic review [16], ergonomic interventions aimed at reducing the negative impacts of sedentary employment include: optimizing the work environment – adapting the workspace to the anatomical, anthropometric, physiological, and biomechanical requirements of the individual; organizational interventions – focusing on optimizing work and rest regimes and other socio-technological requirements; cognitive aspects – considering demands on perception, memory, thinking, and motor response. Żywień et al. [17] estimated the risk of low back pain by comparing the pressure pain threshold of soft tissue and the angles of the spine in young white-collar workers. The results indicated that pressure pain thresholds and the angle of the spine in the sitting position were associated with mild low back pain in female subjects. In addition, mild lower back pain was related to the following in the male participants: angles of the torso; the lumbosacral spine in the corrected sitting position; and body mass index.
Aim of the study
In our study, we delved into the dynamics of muscle activity and working postures among administrative workers. Our primary focus included comparing electromyographic (EMG) muscle activity during uncorrected sitting, corrected sitting, and corrected standing positions. We also explored differences in EMG activity between administrative workers and a control group in various seated and standing conditions. Lastly, we examined the disparities in perceived discomfort between administrative workers and the control group. These key inquiries form the nucleus of our research, offering valuable insights into the intricate relationships between working postures, muscle activity, and perceived discomfort in the workplace. It is difficult to clarify the correlation between specific posture and pain [18,19]. Therefore, we measured EMGs in different postures with the hypothesis that with the forward head posture and the extension of the lever arm that the neck musculature has to neutralize, higher demands are placed on the muscular system and, at the same time, the interosseous connections of the neck face higher loads, which may lead to repetitive strain injury. Considering the needs of the study, we were primarily concerned with local muscle strain in the upper limbs, with the hypothesis of whether EMG may have an influence on emerging upper limb pain conditions or whether the problems are caused by other influences.
Material and methods
Sample
The research cohort comprised 31 participants, evenly split into two groups, aged 30 to 40 years, with an average age of 32.7 years (SD 3.2), aligning with the standard sample size of 10-15 individuals recommended in the majority of EMG studies [6,11]. The sample size was determined by balancing statistical power with practical constraints, including costs and time demands for data collection and analysis. Group A consisted of administrative workers routinely using computers, while control Group B was a randomly selected sample from the general population. Gender distribution in Group A was 8:8 (male:female), and in Group B, it was 9:6. Each group had only one individual with predominantly left-handed lateralization. Exclusion criteria included neurological disorders, documented musculoskeletal issues in the cervical spine and upper extremities, acute cardiorespiratory conditions, congenital abnormalities, or oncological symptoms. Additional exclusion criteria encompassed visual or auditory impairments without optimal correction, a history of significant trauma, or surgery.
Data collection methods
Participants completed a laterality questionnaire [20] and provided basic anamnestic information at the measurement outset. Surface electromyography (EMG) was conducted using Shimmer 3 Ebio Consensys Development Kit devices, with two units affixed above the lateral epicondyles of the humerus. Placement of Kendall adhesive electrodes followed palpation guidance during muscle contraction. The distance between corresponding electrodes on a given muscle was consistently set at 1 cm. Electrode pairs were positioned on the extensor digitorum muscle of the index finger, the flexor digitorum superficialis muscle of the index finger, and the reference electrode above the olecranon fossa of the corresponding arm (Figure 1). Flexible mesh straps were used on the upper extremities to minimize electromagnetic interference. Post-measurement, each participant completed the Body Part Discomfort Assessment Checklist (BPDAC) questionnaire [21], rating discomfort on a scale of 0 to 10, supplemented with verbal comments for non-zero values. A physiotherapist also gathered a relevant medical history during the initial assessment.

Measurement procedure
The measurement commenced with a maximum grip strength test, repeated immediately after the third measurement series for subsequent maximal voluntary contraction (MVC) normalization. Testing was performed sequentially on both upper extremities, with participants standing upright, the tested arm adducted, and the elbow joint at a right angle. EMG measurements occurred in three five-minute series. The first series involved uncorrected sitting with individualized workstation adjustments. In the second series, participants were positioned in a corrected posture adhering to ergonomic standards. The third series took place with participants standing at a Sit-Stand desk with ergonomic corrections.
Data processing
Data preprocessing included ensuring data quality and noise removal from the Shimmer device. Resampling was performed to address Bluetooth-related fluctuations in sampling frequency, resulting in a consistent data file for simplified analysis. Statistical analyses were conducted using RStudio software (version 2023.12.1+402). Initial steps involved rectification and signal filtering (20-400 Hz). Maximal voluntary contraction (MVC) normalization utilized grip strength recordings and resistance tests. Statistical tests applied included the Mann-Whitney-Wilcoxon test for two independent samples with continuity correction for comparing two medians [22] and Welch’s ANOVA for comparing three or more means [23].
Results
Muscle activity
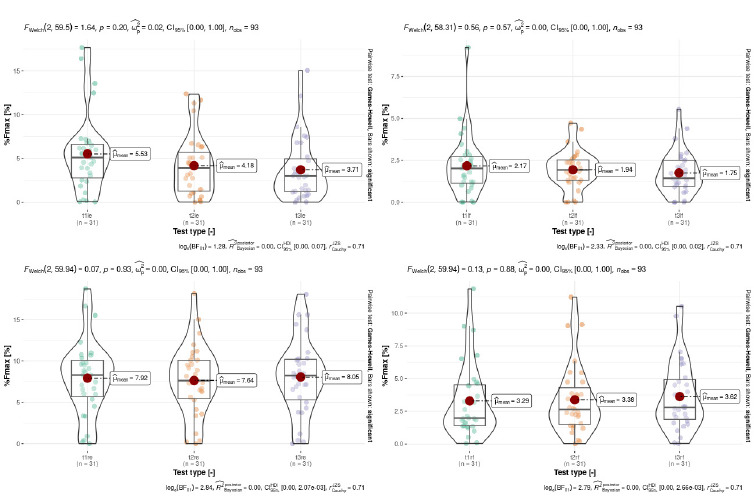
The average activity of the left upper limb extensor during uncorrected sitting was 5.53 (SD=4.38) % Fmax (proportion of maximum voluntary contraction), during corrected sitting 4.18 (SD=3.52) % Fmax, and during corrected standing 3.71 (SD=3.58) % Fmax. For the left upper limb flexor, the averages during uncorrected sitting, corrected sitting, and corrected standing were 2.17 (SD=1.82) % Fmax, 1.94 (SD=1.15) % Fmax, and 1.75 (SD=1.29) % Fmax, respectively. Similarly, the average activity of the right upper limb extensor during uncorrected sitting was 7.92 (SD=4.53) % Fmax, during corrected sitting 7.64 (SD=4.26) % Fmax, and during corrected standing 8.05 (SD=4.57) % Fmax. For the right upper limb flexor, the averages during uncorrected sitting, corrected sitting, and corrected standing were 3.29 (SD=2.82) % Fmax, 3.38 (SD=2.68) % Fmax, and 3.62 (SD=2.61) % Fmax, respectively (Table 1).
Table 1
Descriptive statistics of muscle activity of the extensor digitorum and the flexor digitorum superficialis
[i] Notes: bt_max_r – maximum voluntary contraction (MVC) of the right hand before the test; bt_max_l – MVC of the left hand before the test; at_max_r – MVC of the right hand after the test; at_max_l – MVC of the left hand after the test; t1_wpm – words per minute (WPM) in the first position (uncorrected sitting); t2_wpm – WPM in the second position (corrected sitting); t3_wpm – WPM in the third position (corrected standing); t1le – left extensor in the first position (uncorrected sitting); t1lf – left flexor in the first position (uncorrected sitting); t1re – right extensor in the first position (uncorrected sitting); t1rf – right flexor in the first position (uncorrected sitting); t2le – left extensor in the second position (corrected sitting); t2lf – left flexor in the second position (corrected sitting); t2re – right extensor in the second position (corrected sitting); t2rf – right flexor in the second position (corrected sitting); t3le – left extensor in the third position (corrected standing); t3lf – left flexor in the third position (corrected standing); t3re – right extensor in the third position (corrected standing); t3rf – right flexor in the third position (corrected standing); % Fmax – share of maximum voluntary contraction.
Comparison of EMG activity
Within the scope of this analysis, we aimed to investigate whether there is a difference in EMG muscle activity during uncorrected sitting, corrected sitting, and corrected standing. The Welch’s ANOVA results indicated no statistically significant difference in EMG activity for left finger extensors (p=0.20), right finger extensors (p=0.93), left finger flexors (p=0.57), and right finger flexors (p=0.88). All p-values exceeded the significance threshold (0.05), indicating no statistically significant difference (Figure 2).
Comparison of EMG activity between administrative workers and the control group
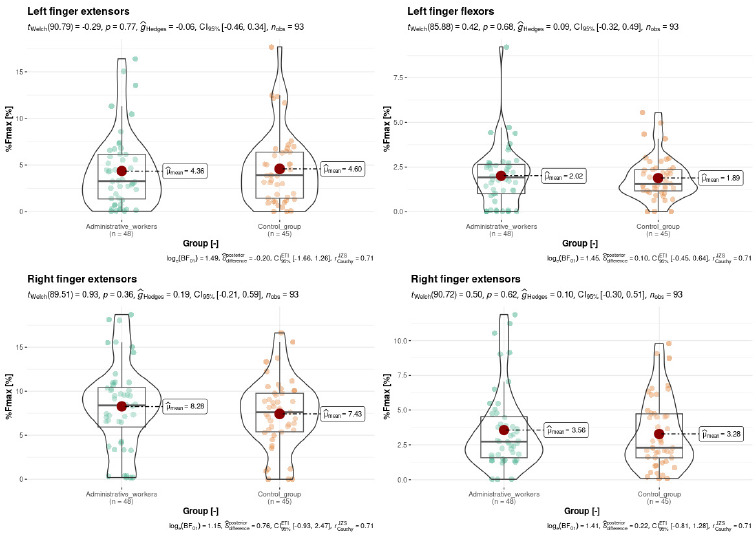
Within the framework of this investigation, our objective was to examine whether there exists a variance in EMG muscle activity between uncorrected sitting and corrected sitting among administrative workers in comparison to the control group. The Welch’s ANOVA results revealed no statistically significant difference in EMG activity between the muscle groups of administrative workers and the control group. For left finger extensors (p=0.81), right finger extensors (p=0.95), left finger flexors (p=0.82), and right finger flexors (p=0.94), all p-values exceeded the significance threshold (0.05), indicating no statistically significant difference (Figure 3).
Comparison of discomfort between administrative workers and the control group
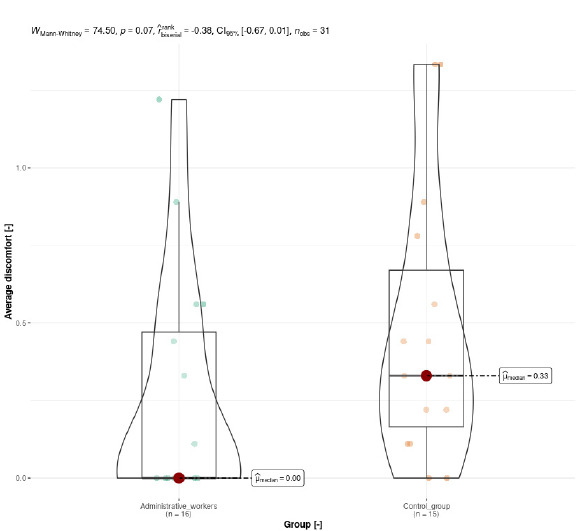
Conclusively, we investigated whether there is a discernible difference in discomfort between administrative workers and the control group. The data is visually presented in Figure 3. The Mann-Whitney-Wilcoxon test, with a continuity correction yield of p=0.07, indicated no statistically significant difference. The control group reported, on average, higher discomfort (median 0.33) compared to administrative workers (median 0) (Figure 4).
Discussion
Within the scope of this study, no difference was observed in the EMG activity of extensors and flexors during uncorrected and corrected sitting or corrected standing. However, these results align with findings from other studies employing similar research methodologies. For instance, Christensen et al. [24] reported a lack of statistically significant differences across four positions, with testing lasting three times longer in a single phase compared to our research. This result might be explained by the theory suggesting that there is no perfect sitting position, emphasizing the importance of variably alternating postures [24]. Therefore, considering factors such as work organization and implementing a work-rest regimen, including frequent short breaks or longer breaks around 15 minutes, may enhance work variability, concentration, and efficiency [25]. Prolonged sitting periods, exceeding 120 minutes, as observed in the study by Baker et al. [5], are not recommended due to a sharp increase in discomfort and cognitive symptoms. In this research, discomfort correlated with fatigue in the musculus obliquus externus abdominis, evidenced by an increase in amplitude or a decrease in the median frequency of the EMG signal.
Another plausible explanation is the adaptation to a habitual sitting posture, disrupted by the correction, suggesting that even though ergonomically corrected sitting may be less energetically demanding, maintaining such an unusual posture requires a higher level of musculoskeletal system activity. This data can also be interpreted through overall higher EMG activity in extensors, indicating their sustained activity during keyboard typing and shifting one’s gaze between the monitor and keyboard. The elevated activity in extensors may be related to the high prevalence of lateral epicondylitis among workers, who are associated with prolonged and strenuous work, forceful tasks, the combination of force and repeated upper limb movements, and activities in unusual settings [26]. However, it is essential not to overlook the synergistic activity of wrist and finger muscles, which, according to Bernstein [27], plays a crucial role in organizing individual muscles or their parts to ensure dynamic stability under various external and internal conditions.
The goal of head ergonomics in sitting is to center all joints to normotone the muscle fibers around the joints in question. In this way, the muscles can stabilize the joints in question, and the muscles are also more able to perform their functions in the best possible way (phasic, postural) [28]. Thus, when sitting, there is more static load on the lumbar and pelvic region than when standing [29]. Sitting can also cause decentration of the hip joints or hyperlordosis (or hyperkyphosis) in the lumbar spine, where the thoracic and cervical spine also respond [30]. The result is decentration of the shoulder joints and altered muscle activation in the upper extremities [31]. When standing, the energy demand is greater than when sitting, mainly due to the activation of the muscles in the lower limbs. During standing, fatigue may cause hyperextension at the knee joints, a tendency to pelvic anteversion, hyperlordosis of the lumbar spine, hyperkyphosis of the thoracic spine and hyperlordosis of the cervical spine. Another sign is a decentration of the shoulder joints and other changes in muscle activation [32,33].
Ergonomic correction should be viewed as a long-term adaptation to biomechanically less demanding settings, with variations introduced throughout computer work time, ideally within a 2-hour interval. Additionally, individuals should engage in nonspecific physical activity to minimize the likelihood of musculoskeletal disorders. The results prompt reflection on the method of verifying the effectiveness of ergonomic interventions. Testing a one-time correction among different groups may not capture its impact, as evidenced by inconclusive or conflicting results in several studies [24,34,35]. Therefore, future studies should consider transitioning the study structure to monitor the impact of ergonomic interventions over time rather than conducting one-time corrections.
This study has notable limitations that demand consideration. The primary constraint is the restricted sample, comprising solely administrative personnel, limiting the generalizability of results and conclusions to other professions or workgroups. Furthermore, the accuracy of EMG muscle activity measurements may be influenced by factors like electrode placement, muscle movements, and individual variability. Another limitation arises from the absence of long-term tracking of ergonomic intervention effects on muscle activity and discomfort perception. A valuable avenue for future research involves a longitudinal study examining sustained impacts on the health of administrative personnel. Additionally, the measurement of surface muscles has inherent constraints, capturing only superficial muscle activity and excluding the monitoring of deep muscles — a notable methodology limitation. It is also important to mention that the body position was not controlled.
Despite these limitations, the study offers significant contributions. Focusing on administrative personnel, prone to prolonged sitting, it provides specific insights into muscle activity within this occupational profile. Comparing various work positions (sitting without correction, sitting with correction, standing with correction) and their impact on muscle activity and discomfort leads to information on practical ergonomic adjustments, ultimately enhancing the health of administrative workers. Moreover, the study contributes to literature addressing the relationship between sedentary employment and health, establishing a foundation for further research in ergonomics and the prevention of ailments associated with prolonged sitting. Despite the acknowledged limitations, this study stands as a valuable addition to ongoing discussions on workplace ergonomics and its broader implications for occupational health and well-being.
Conclusions
Our study concludes that short-term corrections exhibit no discernible impact on EMG activity. Although the investigation falls short of fully elucidating the adaptation dynamics to workstation adjustments and sitting postures in computer-related tasks, a significant correlation emerges. Administrative workers, as the adapted group, manifest lower discomfort levels compared to the control group. This finding underscores the remarkable adaptability of the human body to adverse conditions, particularly evident in participants during the uncorrected sitting phase. It emphasizes the broader notion that adaptability extends across different settings, highlighting the significance of implementing biomechanically fewer demanding configurations. However, the average EMG activity shows no statistically significant difference between administrative workers and the control group. For a comprehensive exploration of the correlation between EMG activity and discomfort, further investigations, such as pressure algometry at different testing phases, are imperative. These efforts are crucial for a nuanced understanding of the intricate relationship between electromyography activity and subjective discomfort within the context of ergonomic interventions.