

Introduction
Rapidly progressive glomerulonephritis (RPGN) is a clinical syndrome commonly presented as accelerated decrease of renal function, microscopic hematuria, subnephrotic proteinuria and histopathological findings of crescent formations in the glomeruli. The most common cause of RPGN in adults is ANCA associated vasculitis (AAV), also known as pauci-immune glomerulonephritis [1]. Although AAV as a type of small vessel vasculitis can be associated with various types of malignancies, its occurrence among patients with solid tumors is extremely rare [2]. Here, we present a case of AAV in a patient with a recurrent pulmonary metastasis of the ovarian malignancy.
Case report
A 69-year-old woman was admitted to our hospital due to deterioration of renal function with complaints of malaise, fever, dry cough and occasional epistaxis that appeared 2 months prior to admission. Over a five-month period, an increase of serum creatinine (sCr) from 130 to 305 µmol/l was noted, followed by severe anemia and urinary abnormalities. A chest radiograph showed postsurgical scars in both lungs with no description of active lung consolidations and no suspected malignant infiltrations. Besides a beta blocker prescribed for sinus tachycardia, she had not taken other medications.
Due to granulosa cell tumor (GCT), our patient was treated with left oophorectomy and postoperative radiotherapy, thirty-nine years before this hospitalization. After fourteen years, she underwent a resection of nine metastases from the left and two metastases from the right lung with adjuvant chemotherapy that included cyclophosphamide, doxorubicin and cisplatin (CAP protocol). One year after that, a resection of one more pulmonary metastasis from the right lung was done, with no evidence of newly formed neoplasms on periodical chest radiograph examinations.
On physical examination she appeared euvolemic, afebrile and normotensive, without rash and oral ulcers. Clinical findings on heart, lungs, abdomen and extremities were normal.
Besides advanced renal failure (sCr 299 µmol/l, estimated glomerular filtration rate [eGFR] MDRD 13.5 ml/min) with a maximal proteinuria level of 3.6 g/day, she had a systemic inflammatory response (C-reactive protein [CRP] 32) and severe normocytic anemia (hemoglobin 68 g/l). Positive p-ANCA were detected in a titer of 1 : 160 with elevated levels of antimyeloperoxidase (antiMPO) antibodies (116 RU/ml). Serum levels of IgG and C4 were slightly increased, while other immunoglobulins and complement component C3 were unremarkable. Besides proteinuria, the urinalysis revealed massive hematuria and leukocyturia with sterile urine culture. Ultrasound examination revealed normal kidney size with mild hyperechogenic parenchyma. We initiated therapy with dual blockade of the renin-angiotensin-aldosterone system (fosinopril, spironolactone) along with a loop diuretic. Due to the above findings, a kidney biopsy was performed.
Histopathologic findings of the kidney biopsy specimen showed cellular crescent formations in all 10 glomeruli, with two completely sclerotic glomeruli and three of them had focuses of initial mesangial sclerosis. Tubulointerstitium was infiltrated with mononuclear cells and foamy transformed histiocytes. Half of the tubules were significantly atrophic with extremely dilated lumens filled with PAS positive material. Blood vessels had thicker walls with mononuclear infiltration. The immunofluorescence microscopy showed discrete C3 staining positivity along the glomerular basement membrane and negative staining for immunoglobulins.
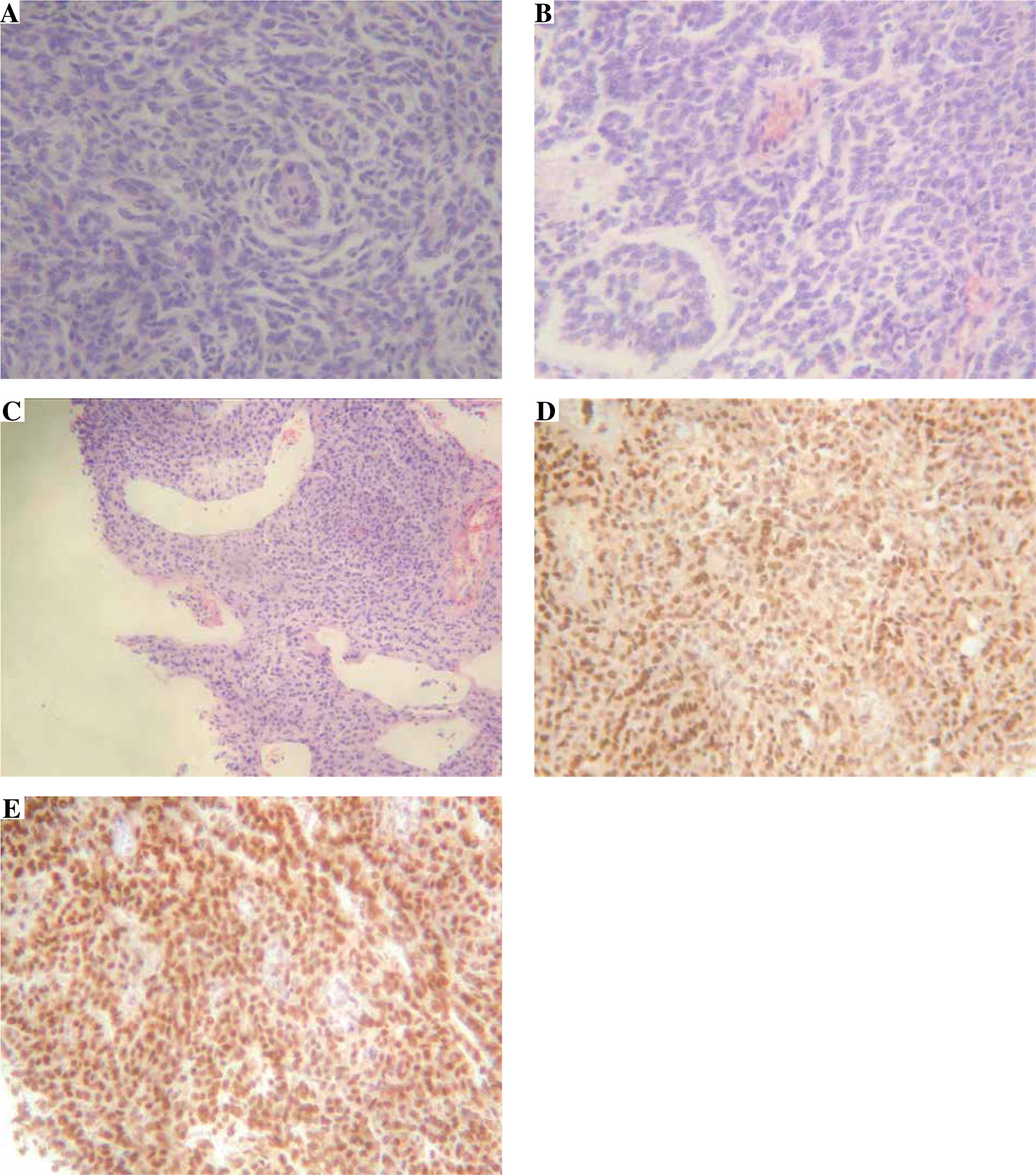
According to the protocol for the treatment of ANCA-associated crescentic glomerulonephritis, normal lung radiography findings and the fact that our patient did not have any clinical manifestations of recurrent lung malignancy, the initial plan was to administer corticosteroid pulses (methylprednisolone 500 mg during three consecutive days) and cyclophosphamide followed by prednisone 60 mg/day. On the third day of corticosteroid pulses, thoracic multislice computed tomography (MSCT) with contrast revealed an irregular shaped soft tissue neoplasm 40 × 48 mm in the posterior-basal segment of the right lung, partly located in the scar with surgical junctions. Computed tomography of the abdomen and pelvic region was clean, without intraperitoneal metastases, and gynecologic examination under the speculum showed normal findings. Due to a high suspicion of secondary glomerulopathy, instead of continuing the protocol with cyclophosphamide we directed our patient to an oncologic council for management of recurrent malignant disease. In the meantime, histopathologic staining of the specimen, provided by ultrasound-guided percutaneous transthoracic biopsy, confirmed the typical, mixed pattern of GCT that was predominantly solid and partly cystic (Fig. 1).
Fig. 1
Various, mixed pattern of GCT: A, B) Microfollicular, trabecular, tubular, diffuse, mimicking carcinoids in some fields, H&E 20×; C) Some parts of tumor are predominantly cystic and filled with clotted blood, H&E 10×; D) All cell expressed estrogen, nuclear positivity 20×; E) All cells expressed progesterone, nuclear positivity 20×
After discharge from the hospital, no further deterioration of chronic kidney disease was detected and prednisone was discontinued after slowly tapering over the next three months (20 mg/month). Oncologic council recommended initiation of treatment with the PEB protocol (cisplatin, etoposide and bleomycin) after nephrologist approval. Due to cisplatin nephrotoxicity and a possibility for simultaneous treatment of malignancy and ANCA associated glomerulonephritis that might not be related to the existing malignancy, instead of PEB our suggestion was to initiate therapy with reduced doses of the CAP protocol that includes cyclophosphamide. As far as we know, the patient was followed up without further deterioration of renal function. She received three cycles of the CAP protocol followed by deterioration of her general condition and a lethal outcome one year after onset of vasculitis symptoms.
Discussion
The incidence of crescentic glomerulonephritis (GN) among patients subjected to renal biopsy is estimated at about 13% and AAV as its most common form accounts for 60-80% of all cases. AAV usually appears as a primary vasculitis that encompasses mainly two subentities: microscopic polyangitis, granulomatosis with polyangitis, and rarely eosinophil granulomatosis with polyangitis [1]. Besides these, other causes such as infectious agents, drugs, connective tissue diseases and malignant diseases can also be triggering factors for AAV development [2].
Malignancy-associated vasculitis occurs in 5.2% of all vasculitis cases registered in the French vasculitis study group database during a period of ten years [3]. Although this type of vasculitis is predominantly described among hematologic malignancies, such as myelodysplastic syndrome and lymphoid malignancies, some solid tumors can also be associated with occurrence of vasculitis. The most common vasculitides seen in malignancies are cutaneous leukocytoclastic vasculitis and polyarteritis nodosa [2, 3]. Unlike these types of vasculitis, ANCA vasculitis have been considerably less often described with solid neoplasms. In a retrospective study conducted by French authors, ANCA was discovered in 20.4% of 44 patients with vasculitis-associated malignancies [3].
We found several published cases with simultaneously diagnosed ANCA vasculitis and solid tumors, mainly lung and gastrointestinal cancers, that had clinically presented as RPGN [4-6]. As far as we know, in patients with ovarian cancer there has been described only one case of leukocytoclastic vasculitis [7] and this is the first case representing ANCA vasculitis associated with any type of gynecological malignancy.
Our patient had a recurrence of the ovarian GCT, a sex cord stromal tumor, that has an incidence of 2-3% among all ovarian cancer patients [8]. Besides slow growth and local spread, one of the main characteristics of GCT is its late recurrence, with the median time interval to the first relapse from 53 to 61 months [9, 10]. Recurrent disease commonly occurs in the peritoneum and pelvis, and rarely in other locations such as lungs and bones [8]. In our case, the second recurrence in the lungs was revealed 39 years after initial treatment and 24 years after the first relapse.
A possible theoretical link between malignancy and ANCA vasculitis is that some cancer cells express granulocyte colony stimulating factor (G-CSF) and initiate neutrophils to produce neutrophil extracellular traps (NETs) in peripheral blood vessels with consequent vascular dysfunction and systemic inflammation [11]. Among chromatin and histones, other proteins including MPO have been identified in NET formations [12]. Thus, NETs are involved in a vicious cycle by stimulating production of anti-MPO antibodies that are able to induce neutrophil activation and degranulation. This results in abnormal cytokine synthesis and release of reactive oxygen species and lytic enzymes that lead to even larger vascular endothelial injury with more NET formation [13].
There might also be a possibility that in our case these two diseases are unrelated. A suspicion of paraneoplastic glomerulopathy is justified when there exists a temporal relationship between the two diagnoses [5]. Although in our case there was a clear temporal relationship between diagnosis of GCT and AAV, considering the slowly progressing growth of GCT it is possible that the tumor had been present long before manifestation of AAV. Besides that, our patient was in the age group between 65 and 74 years, which is reported to be the peak incidence rate age group for diagnosis of AAV [14].
Although ANCA-associated pauci-immune glomerulonephritis implies a glomerular disease without complement and immunoglobulin deposits, these findings are not rare. In our case kidney specimen immunofluorescence findings showed C3 staining positivity that can be found in about one third of glomerular capillary walls of ANCA-associated glomerulonephritis renal biopsy specimens [15]. It is reported that patients with positive glomerular C3 staining have higher rates of proteinuria and poorer initial renal function than those without C3 deposition. These manifestations can be related to a significantly lower percentage of normal glomeruli with more crescentic formations in those patients [15, 16]. On the other hand, a retrospective study that followed patients with MPO ANCA-associated glomerulonephritis for 15 months did not find differences in renal survival between < 2+ C3 intensity staining and ≥ 2+ intensity staining [17].
In our patient, a late relapse of GCT was diagnosed after manifestation of ANCA-associated crescentic GN. Considering the dimensions of the neoplasm described on MSCT and the well-known slowly growing nature of GCT, we concluded that the tumorous mass in the right lung, although not detected on the initial radiographic examination, existed long before development of AAV. In every patient with newly diagnosed vasculitis, special attention should be given to anamnestic data of previous malignant diseases, and according to that clinicians should be focused on exclusion of relapse, especially in the lungs.