

 POLSKI
POLSKI







Introduction
The burden of non-communicable diseases (NCDs) is rising at an unprecedented rate worldwide, becoming the main health concern for society and national governments [1]. The latest evidence highlights that an unhealthy diet and poor nutrition status are some of the modifiable behavioural risk factors responsible for NCDs development [2, 3]. In recent years, the Western diet (WD), based on saturated fats, refined carbohydrates, and salt, has become a modern dietary pattern in many countries. Increased consumption of ultra-processed foods (UPF) may promote low-grade inflammation and thus favour the development of diet-related NCDs, including obesity, cardiometabolic diseases, many cancers, and respiratory and autoimmune disorders such as autoimmune thyroiditis or arthritis [4].
There is also growing evidence that nutrition elements are closely related to autoimmune diseases such as Hashimoto’s thyroiditis (HT). High iodine consumption and inadequate intake of selenium, iron, proteins, dietary fibres, and unsaturated fatty acids may lead to the development of HT [5]. In addition, food having pro-inflammatory properties may promote intestinal imbalance, bacterial overgrowth, rise in intestinal permeability, and oxidative stress, and this all together may lead to enhanced inflammation and consequently increase the incidence of HT [6]. Interestingly, recent data suggest that chronic inflammation is also linked to the development of mental disorders. From baseline to the end of the study period, dietary patterns and levels of inflammatory biomarkers were assessed in all participants. At the age of 18 years, depression risk grew as the inflammatory status increased, highlighting that a diet rich in processed food may raise depression risk in early adulthood [7].Then, introducing a diet rich in antioxidants may help reduce low-grade inflammation and, as a consequence, prevent many NCDs in childhood [8]. Anti-inflammatory diets have origins dating back centuries; however, their meaning in disease treatment and prevention is relatively new. Examples of anti-inflammatory diets include a traditional Mediterranean diet (MD), the Dietary Approaches to Stop Hypertension (DASH) diet, and traditional Okinawan, Nordic, or Mexican diets. The concept of these diets has common core foundations and recommendations. Anti-inflammatory diets are generally based on plant-based foods, including vegetables, fruits, whole grains, nuts, and seeds. These food components provide antioxidants, significant amounts of fibre, as well as vitamins and minerals. Protein is sourced from legumes and lean proteins such as fish and chicken, while healthy monounsaturated fats are derived from olives or nuts. There is also a low intake of saturated fats, which are often present in red meat, and smaller amounts of dairy or alcohol consumption [9, 10].
The family environment from early childhood plays a particularly important role in shaping healthy eating patterns of children and youths. Many variables within the family setting can affect children’s eating behaviour, including their parents’ eating behaviours, foods made available to children, and the child-feeding strategies utilised. Parents’ nutrition knowledge, attitudes, and dietary practices are imperative in preventing the development of NCDs and improving their children’s health as their primary guardians [11].
The present work aimed to assess parents’ and/or legal guardians’ awareness of the anti-inflammatory diet.
Material and methods
The survey on caregivers’ awareness regarding an anti-inflammatory diet was conducted among 326 parents and/or legal guardians of Polish children from the general population between November 2023 and February 2024. Parent participants met the following inclusion criteria during recruitment: having a child, consent to the study, and proper questionnaire completion. Data for the study were collected anonymously using the Computer-Assisted Web Interview (CAWI) method. CAWI is an Internet surveying technique in which the respondent follows a script provided on a website. An anonymous online questionnaire was distributed on forums and discussion groups designed for parents.
The research tool was the author’s questionnaire containing a summary of 22 questions: 7 questions concerning sociodemographic data of the parent (gender, age, education, number of children, height, and weight) and child (age, height, and weight). The questionnaire contained 15 questions about knowledge and use of an anti-inflammatory diet. The questionnaire consisted of closed questions, single and multiple-choice. It also included open questions requiring an answer in 2–3 sentences, which at the same time were checking questions. A pilot study was conducted before the described study. It was conducted twice among the same group of 20 parents with a one-month interval to avoid the freshness effect. The surveyed women had no comments on the questionnaire, and the results obtained from the 2 surveys were reproducible. To assess the reproducibility of the results gained by the questionnaire, the κ parameter was calculated for each questionnaire question (results obtained in the pilot study and after one month). For 71.5% of the questions a very good (κ ≥ 0.80) concordance of answers was obtained, and for 19.2% of the questions a good (0.79 ≥ κ ≥ 0.60) concordance of methods was obtained. For 9.3% of the questions in the questionnaire analysed, the concordance between the results obtained in the baseline and repeat test was moderate (κ < 0.59). Cronbach’s α coefficient for the standardisation sample was 0.91, indicating the selected questions’ high reliability. For the analysis of the collected data, the following software programs were used: Profitest, Microsoft Office Word, Microsoft Office Excel, and Statistica 13.0. The χ2 test was used for statistical analysis, and s, the significance level, was assumed to be p < 0.05.
Results
From the total cohort, 325 participants property completed the provided questionnaire. One caregiver was excluded from the study due to failure to answer questions. The study group was predominantly female (n = 310; 95.4%), aged 31–40 years (n = 238; 73.2%), with higher education (n = 271; 83.4%), normal BMI (n = 211; 64.9%), and 2 children (n = 165; 50.7%). The mean age of children was 5.0 years, while their mean height was 114.2 cm. The characteristics of the study population are shown in Table I.
Table I
Characteristics of the study group
In a question testing the knowledge of the inflammation process, most respondents (n = 300; 93.3%) defined inflammation as a defence mechanism of the body against infection, injury, or tissue damage. Some participants answered (n = 10; 3.1%) that inflammation is an unnatural and unnecessary process, while 2.2% (n = 7) did not know the correct answer. Detailed responses of the study group are summarised in Table II.
Table II
Answers to the question “What is inflammation?” – answers among surveyed parents
In response to the question regarding the basics of an anti-inflammatory diet, most caregivers (n = 265; 81.6%) indicated that such a diet should include antioxidant-rich foods. However, some participants thought an anti-inflammatory diet requires following strict rules on macronutrient intake (n = 18; 5.5%), while 12% (n = 39) of the enrolled parents showed poor knowledge of this diet. Answers given by the participants are presented in Table III.
Table III
Answers to the question “What is an anti-inflammato-ry diet?” – answers among surveyed parents
Among those surveyed, more than half (n = 189; 51.2%) chose the MD as a good example of an anti-inflammatory diet; the second choice was a gluten-free diet, which was indicated by 23.1% (n = 75) of respondents. Interestingly, around 15.1% of participants did not give any answer. Chosen examples of anti-inflammatory diet are presented in Table IV.
Table IV
Answers to the question “Which of the following is an anti-inflammatory diet?” – answers among surveyed parents
| In your opinion, which of the following is an anti-inflammatory diet? | n | % |
|---|---|---|
| Gluten-Free diet | 75 | 23.1 |
| Juice diet | 6 | 1.8 |
| Mediterranean diet | 189 | 58.2 |
| Low energy diet | 6 | 1.8 |
| I don’t know | 49 | 15.1 |
In answer to the question of which of the following was an anti-inflammatory diet, 189 (51.2%) parents indicated the MD, and 75 (23.1%) chose a gluten-free diet. A juice diet and a low-energy diet was indicated by the same number of people (n = 6; 1.8%). However, 49 (15.1%) respondents did not know the answer.
Most of the recruited caregivers (n = 165; 50.8%) admitted that they had an unsatisfactory level of knowledge about the anti-inflammatory diet, whereas 30% (n = 66) and 5.5% (n = 16) described their recognition level of this diet as good and excellent, respectively. However, most respondents (62.8%, n = 204) did not know what kind of food should be included in an anti-inflammatory diet. Figures 1A and 1B present the detailed answers.
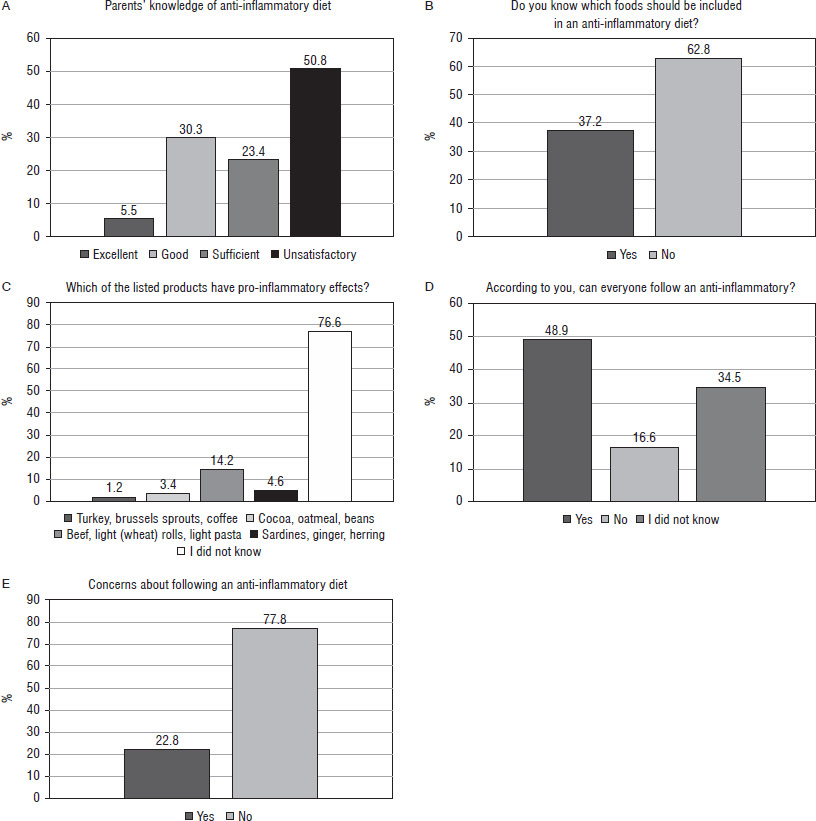
Moreover, 76.6% (n = 249) of participants could not choose listed natural products with anti-inflammatory activity (Fig.1). Interestingly, even though most of the surveyed persons had a poor understanding of an anti-inflammatory diet, almost 50% (n = 159) believed that everyone could follow such a diet, and nearly 80% did not show any concerns regarding this diet (Fig. 1).
On the other hand, there was a statistical relationship between the willingness to implement an anti-inflammatory diet and the respondents’ knowledge level. Those with insufficient knowledge were more reluctant to introduce an anti-inflammatory diet (p > 0.05) (Table V).
Table V
The relationship between the willingness to implement an anti-inflammatory diet and the respondents' knowledge level
Over half of the parents participating in the survey obtained information about child nutrition from the Internet (n = 169; 51.7%). Other popular sources of knowledge indicated by caregivers included books (n = 119; 36.6%), research articles (n = 87; 26.8%), and dieticians (n = 80; 24.6%). Respondents were least likely to obtain their knowledge from family members (n = 23; 7.1%), an educator (n = 12; 3.7%), or a nurse (n = 5; 1.5%). Table VI presents the most popular sources of nutritional knowledge among caregivers.
Discussion
An anti-inflammatory diet plays a crucial role in reducing the burden and preventing many NCDs in childhood [8]. For example, a large prospective cohort study comprising 6,939 children aged 8.5 years, free of depression at the time of recruitment, and followed for 10 years, has shown the association between a pro-inflammatory diet and depression occurrence [7]. Beyond the individual child characteristics, the family environment is important in shaping children’s relationship with food, and the impact of parent’s modelling behaviour cannot be overstated. Parents’ attitudes, beliefs, and dietary practices are fundamental in developing chronic inflammatory-related diseases in children. Children’s first nutrition educators are their parents, who pass on nutrition behaviours to them. Parental beliefs and dietary practices are key in creating and strengthening children’s eating habits and behaviours Parents’ level of education also affects their ability to process health-related information, and as a result, they make better health-related decisions. New information inspires them to adopt healthy lifestyles as role models for their children [13, 14].
In the presented study, more than half of the respondents surveyed (50.8%) admitted that their recognition of an anti-inflammatory diet is unsatisfactory. Moreover, those with insufficient knowledge of healthy eating habits were less willing to change their children’s diet. Therefore, nutrition education should promote desirable nutritional practices and shift towards emphasising eating patterns instead of single nutrients or foods. Greater parental nutritional education can affect a child’s health for a lifetime. A recent study conducted among 302 mothers has shown that higher parental nutritional knowledge was positively associated with the normal weight of their children. Mothers with higher awareness of the impact of diet on the child’s health chose better quality products such as vegetables, fruit, and legumes than those with poor education levels [15]. Moreover, unhealthy eating habits were observed in families with lower parental education levels and socioeconomic status [16]. For example, the study on 365 children aged 8–12 years, investigating the association between the Dietary Inflammatory Index and cardiovascular health, showed that a more pro-inflammatory diet significantly increases the likelihood of developing hypertension and obesity. Moreover, unhealthy eating habits were observed in families with lower parental education levels and socioeconomic status [16].
Recent data emphasise that there is an association between nutrition label use and dietary quality attributable to nutrition knowledge; individuals reading product labels have higher nutritional awareness than non-label users [17]. Moreover, nutrition label use provides an extra advantage regarding dietary intake beyond the effects of nutrition knowledge. Label users consume less total fat, saturated fat, cholesterol, and sodium [18]. Also, there is evidence that proper reading of food labels helps maintain optimal body mass. Parental use of nutrition labels to make healthier food choices has resulted in a lower probability of overweight or obesity in children [19]. Such findings emphasise that higher parental nutritional knowledge and healthy eating habits in the family can effectively reduce the burden of obesity and other long-term NCDs. Nonetheless, only a few caregivers have an understanding of obesity and its consequences. Only 11.3% of parents surveyed in the study aiming to assess caregivers’ level of awareness of obesity agreed that promoting healthy eating habits and regular physical activity protects against abnormal weight development [20].
Our results also indicate the need for parental education regarding proper dietary patterns. Interestingly, in this study, most caregivers (81.5%) pointed out that an anti-inflammatory diet should contain products with antioxidant activities. However, only 58.2% chose MD as a good example of such a diet. Moreover, 62.8% and 76.6% of participants had difficulty selecting food and single products with anti-inflammatory properties, respectively. Similar conclusions were drawn based on the study exploring the level of knowledge in Polish mothers regarding programming and its relationship with children’s nutrition. The cohort included in this study comprised 363 women aged 20-43 years, with children under the age of 3 years. Participants were asked to complete the questionnaire, testing their recognition of nutritional programming, nutrition during pregnancy, and their children’s nutritional intake. Alarmingly, only 44% of respondents correctly defined the term ‘nutritional programming’; moreover, most of the mothers had insufficient knowledge about dietary recommendations for children. Interestingly, those with lower education overestimated their understanding of healthy dietary patterns [21]. Finally, our study demonstrated that the Internet is the preferred source of information on nutrition facts, followed by books, research articles, and dieticians. However, some research has shown that online nutrition information is commonly inaccurate and of low-quality. Caregivers seeking information on the Internet risk being misinformed [22]. This finding indicates there is a need for increased reliability of online nutrition-related information by improving and controlling the nutritional content of specialists. Surprisingly, this study showed that medical health providers are not favourable sources of nutritional knowledge. Dietitians are the most appropriate source of nutritional information; however, other health professionals should be able to provide top-quality nutrition care. It also includes general practitioners (GPs) in primary health care to give a productive nutrition consultation to their patients. Nevertheless, research data show that GPs lack self-confidence in nutrition consulting [23]. Therefore, implementing effective nutrition education and policies aiming to overcome barriers and improve the nutritional knowledge of GPs seems to be a key to the quality and quantity of nutritional counselling. The presented results align with other studies investigating caregivers’ awareness of children’s proper nutrition. Therefore, improving parental nutritional awareness is a fundamental prerequisite for preventing long-term NCDs. Education, guidance, counselling, training, and other approaches are imperative in strengthening their nutritional cognition, with the goal of enabling them to integrate this knowledge into their daily dietary habits. Moreover, nutritional education should be addressed not only to parents/caregivers but also to other family members and teachers.
Limitations of the study
The study cohort predominantly comprised female participants. The authors’ failure to obtain data on equality from fathers and mothers limited this study in that respect.
Using only social media to provide the questionnaire may affect the representativeness of the group and, therefore, interfere with the outcomes. Even though the online survey was an attractive tool, access to the Internet and social media also limits the choice of potential research participants.