




Primary cardiac tumors are rare in the general population (0.002%), with benign neoplasms accounting for 9 out of 10 cases, myxomas being the most common form. However, cardiac hemangioma (CH) described in this case is very rare and occurs as a single tumor in less than 3% of cardiac tumor cases [1].
A 50-year-old woman with newly diagnosed hypertension presented to the cardiology outpatient clinic complaining of dizziness and intermittent palpitations without abnormalities on physical examination and laboratory tests. Transthoracic echocardiography (TTE) revealed an abnormal mass in the right atrium (Figures 1 A, B). The patient was referred to the hospital for transesophageal echocardiography (TEE).
Figure 1
Transthoracic and transesophageal echocardiography views of tumor in right atrium. A – Transthoracic echocardiography view. B – Visual presentation of mutual relations between tumor (blue ring) and atrioventricular node (yellow circle). C – Transesophageal echocardiography view
AO – aorta, LA – left atrium, LV – left ventricle, PFO – patent foramen ovale, RA – right atrium, RV – right ventricle, *cardiac hemangioma.
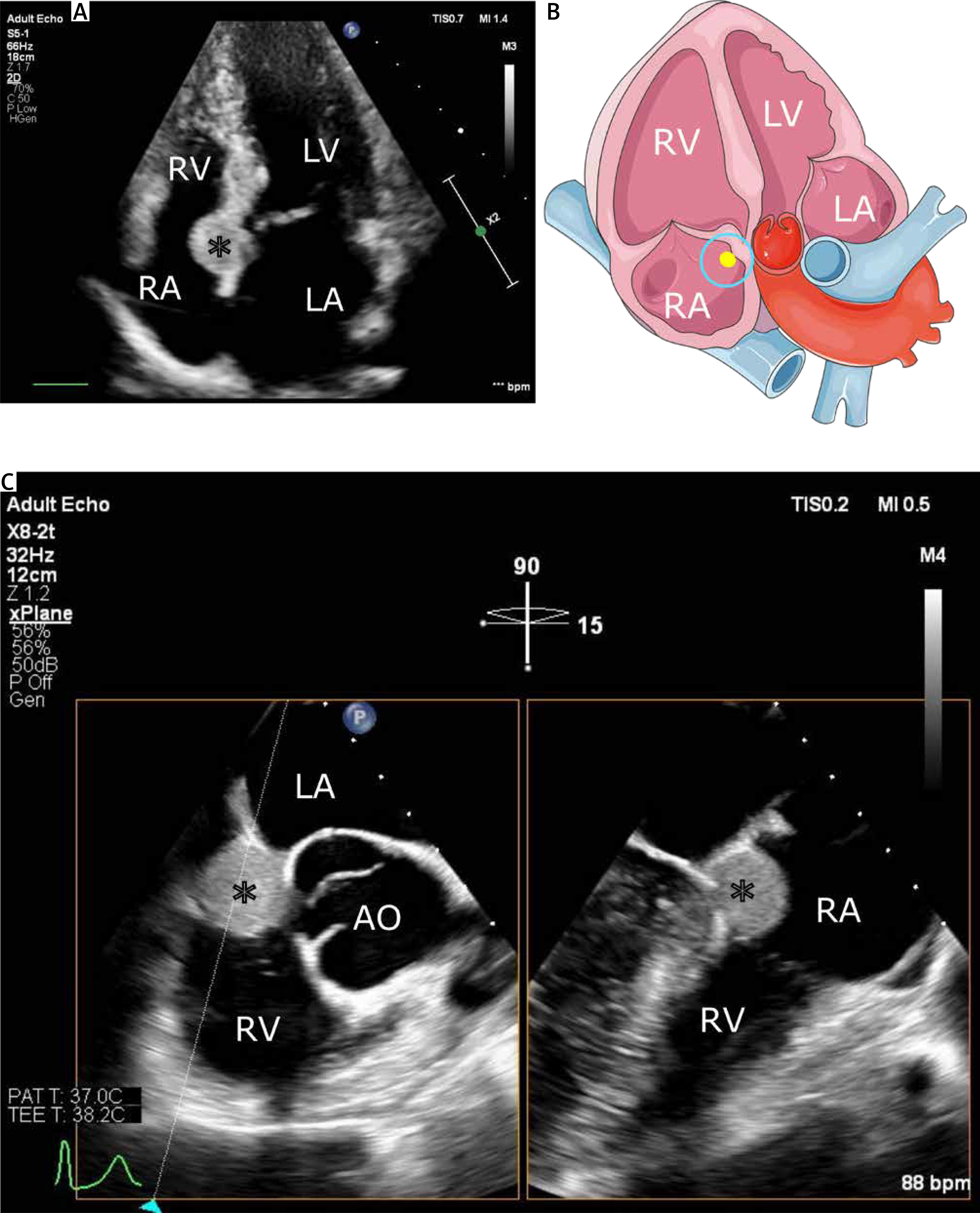
An inpatient TEE confirmed a mass of 20 × 18 mm with sparse mobility (Figure 1 C) and patent foramen ovale. The initial diagnosis of a benign cardiac tumor was made, and because of the diagnosed complete atrioventricular block, the patient was urgently admitted to the Department of Cardiac Surgery. Chest radiography and coronary angiography revealed no abnormalities.
The woman underwent surgery with the use of extracorporeal circulation, general hypothermia of 32°C, and blood cardioplegia. Intraoperatively, a solid tumor (20 × 18 mm) was found between the tricuspid valve, coronary sinus, and aortic valve (Figure 2 A). The mass was removed along with a fragment of the right atrial wall (Figure 2 B). Atrial septoplasty with patent foramen ovale closure was performed. The temporary epicardial leads were sutured.
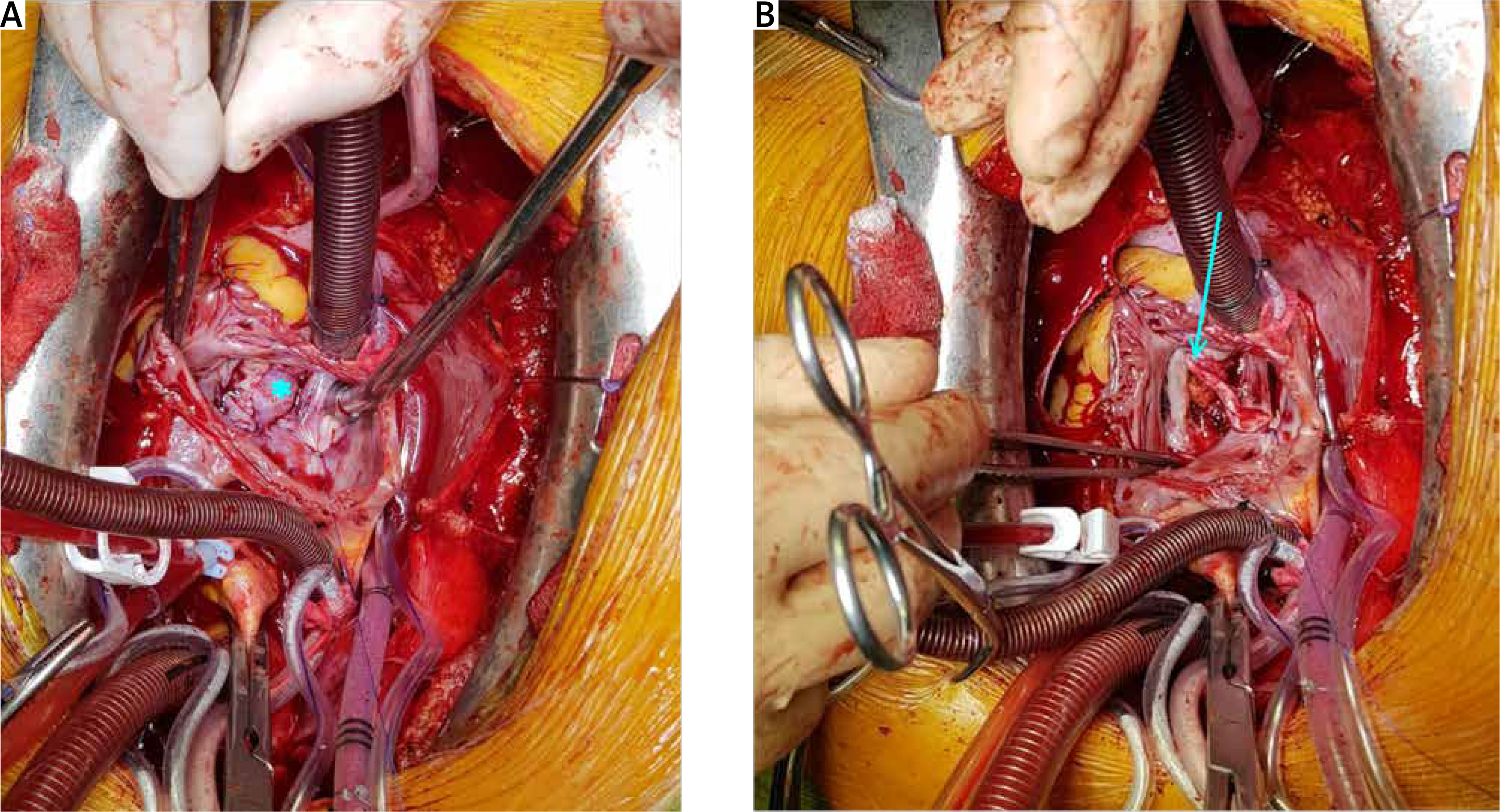
Figure 2
Intraoperative photos. A – Visible hemangioma (indicated by blue *) in the right atrial lumen. B – The lodge after tumor removal (indicated by blue ↓)
After surgery, the patient-paced heart rate was 80/min due to a sustained third degree atrioventricular block. The result of histopathological examination revealed a cardiac hemangioma. An Abbott SJM Tendril STS 2088TC endocavitary lead with a length of 58 cm was implanted in the middle of the septum and then connected to the Medtronic Sensia pacemaker. The pacemaker was examined after implantation and a TTE was performed. No abnormalities were detected. The patient was discharged to a rehabilitation unit.
At the 1-month follow-up, the patient was in good condition and showed no further symptoms. The patient is under further observation by the cardiology and cardiac surgery outpatient clinic.
Cardiac hemangioma can develop at any age, but on average it occurs in patients around the age of forty and is approximately 4.5 cm in size. Coronary angiography shows tumor blush or abnormal vessels around the tumor in one-third of CH cases [1]. Treatment includes resection of the tumor with complete ligation of its vessels. Long-term complications of surgical treatment occur in 3.5% of patients, more commonly in patients undergoing biopsy or low-impact surgery. [1]. When resection is not possible, conservative treatment with propranolol have been reported in the literature [2, 3].
Cardiac hemangioma is a benign tumor originating from endothelial cells and consisting of limited proliferation of small blood vessels. Microscopically, vascular channels with a single layer of endothelial cells can be seen. The histologic appearance may vary depending on the type of cardiac hemangioma. The most commonly described type is cavernous hemangioma with characteristic hyperexpanded vessels and thin walls. In some cases, the vessel walls may be thickened due to fibrosis [4]. Capillary-type cardiac hemangioma consists of small capillary-like vessels [5]. The last and least common type, arteriovenous, consists of thick-walled dysplastic arteries, veins, and capillaries with poorly defined boundaries [6]. The cardiac hemangioma types may coexist within the tumor. The histologic type of the tumor does not affect treatment methods [1].
Most patients are asymptomatic, but symptoms if they are present might include a decreased exercise capacity, syncope, or angina. Hypertension detected in patients is one of the elements that frequently coexist with CH [1]. The absence of abnormalities in coronary angiography sometimes complicates or extends the proper CH diagnosis.
The anatomical location of CH indicates that the tumor was the primary cause of persistent third degree atrioventricular block due to damage to the atrioventricular node. Because of the radical removal of CH, no further treatment was considered, suggesting that the patient had fully recovered from this cause. Cardiac hemangioma may be one of the rarest causes of this arrythmia, but should always be considered as one of the possible reasons for an AV block.