




Chest wall tumours are uncommon lesions, with an incidence of less than 2% of paediatric solid tumours. Overall, the majority of chest wall tumours are malignant and belong to the family of small round blue cell tumours of the Ewing’s family of primitive neuroectodermal tumours. The literature has few large case series in view of their rarity of occurrence in children. From a management point of view, the bony chest wall provides a challenge to complete excision of the tumour and subsequent reconstruction [1]. Against this background, the interesting presentation and management of a massive chest wall tumour with dumbbell extension in a child is detailed.
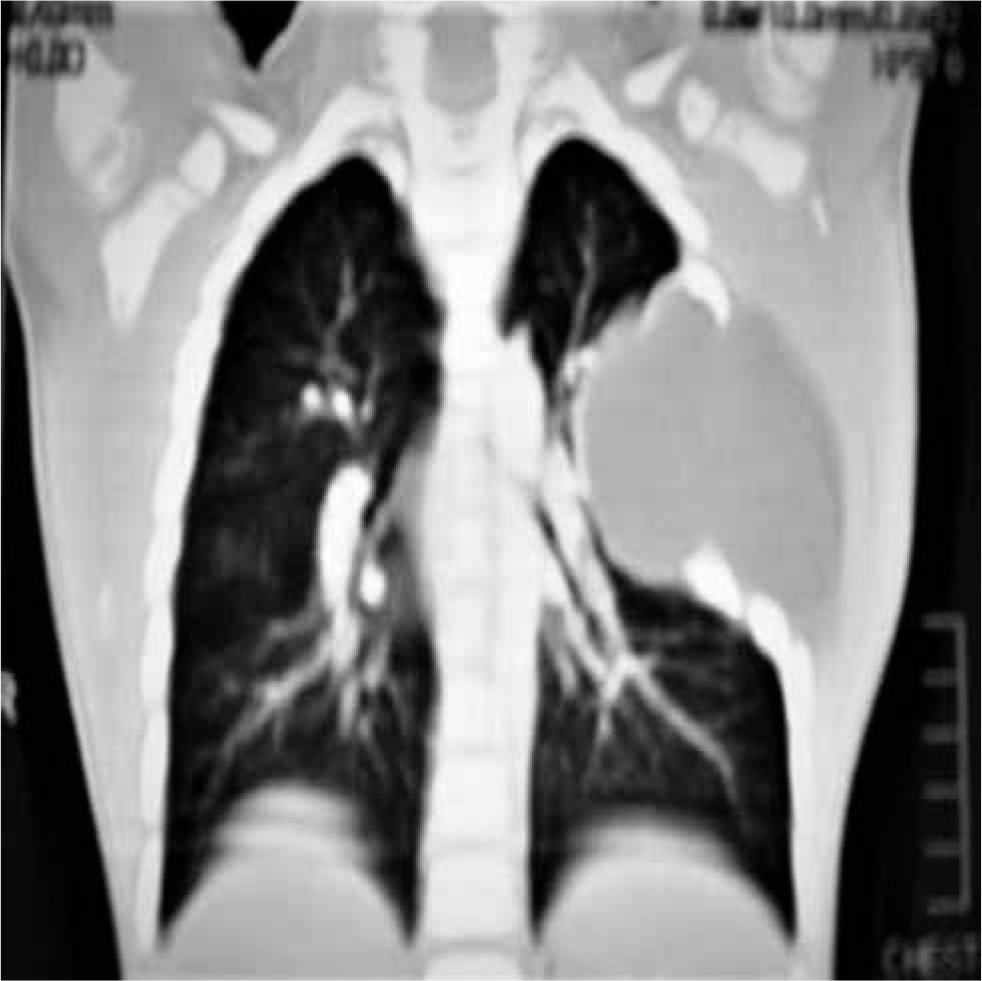
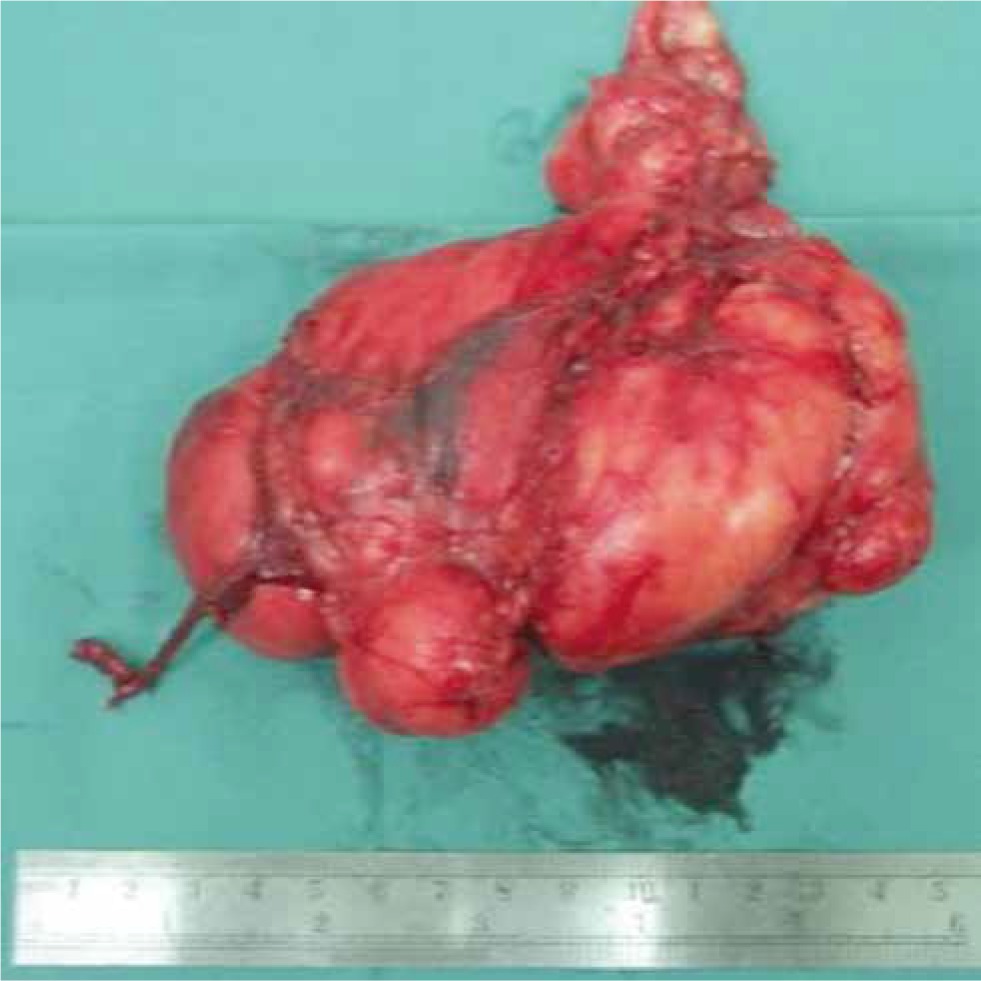
A 7-year-old boy presented with a left chest swelling, noted since the age of 2 years. In view of a recent increase in size of swelling over the past year, the parents sought medical attention. The boy was otherwise well, without any local pain or discomfort over the swelling. On local examination (Figure 1), a non-tender firm swelling measuring about 7 × 6 cm was palpable over the antero-lateral left lower chest wall, extending into the axilla. The skin over the swelling appeared normal without any prominent vessels. No distal neurovascular deficit was observed in the left upper limb. The systemic examination was unremarkable. Plain X-ray of the chest revealed a soft tissue density with concave deformity of the underlying 4, 5, 6 ribs without bony erosion on the left side. Further imaging with computed tomography (CT) contrast of the chest identified the swelling to be non-enhancing, uniformly homogeneous with density consistent with adipose tissue. The swelling appeared to be encapsulated, dumbbell shaped with the deeper part extending between the ribs to reach the lung hilum subpleurally (Figures 2, 3). Fine needle aspiration cytology of the swelling was consistent with adipose tissue. A preliminary diagnosis of benign chest wall tumour was made and surgical excision was undertaken after obtaining informed written consent. Intraoperatively, the swelling was posterior to the intercostal muscles and anterior to the pleura with a dumbbell extension into the 4th intercostal space, without adherence to the pleura. The swelling was excised completely. After excision, the swelling measured 8 × 6 cm, yellowish, firm, lobulated with a dumbbell appearance (Figure 4). Histology confirmed the presence of mature adipose tissue interspersed with fibrotic strands, consistent with a fibrolipoma. After excision, he made an uneventful recovery and was discharged home on day 2 with analgesics. He is well without recurrence at 2-year follow-up after excision.


Masses arising in the chest wall are reportedly malignant in most adult as well as paediatric series varying from 50% to 70%. Any chest wall lesion is viewed with suspicion until proven otherwise by histopathology. Against this background, benign tumours of the chest wall assume importance in that they are uncommon lesions in practice.
Benign chest wall tumours include haemangioma, hamartoma, fibromatosis. eosinophilic granuloma, aneurysmal bone cyst, hamartoma, osteoma, osteochondroma, and chondroma. Pain may be the presenting symptom in bony tumours due to periosteal stretching, whereas soft tissue tumours may be asymptomatic in the child. Due to the absence of symptoms, soft tissue tumours assume large sizes before being noted by parents. Asymptomatic occurrence with detection due to X-ray evaluation for respiratory tract infection is one of the modes of presentation. Also, trivial trauma can bring these soft tissue tumours to medical attention. Accurate differentiation between benign and malignant chest wall lesions may not be possible on clinical examination. However, large size, sudden increase in size, pain, fixity to the surrounding structures, and bony erosion are pointers to malignancy [2, 3]. With regard to evaluation of these lesions CT and magnetic resonance imaging (MRI) have been proposed as imaging options. CT is useful in the delineation of the lesion for surgical planning, extent of bony, soft tissue, and mediastinal involvement. MRI scores over CT in cases of vascular and neural involvement, especially spinal cord extension. Motion artefacts, sedation, and long acquisition time are supposedly factors not favouring MRI [2]. Cytology by needle aspiration is helpful in ascertaining the nature of the lesion pre-operatively although accuracy may vary depending on the sampling technique. To augment the value of cytology, image-guided aspiration is a valuable tool.
In the case of malignant chest wall tumours, reconstruction is a formidable task, but the general principles include maintenance of chest wall integrity and functionality by appropriate prosthetics. En bloc excision with tumour-free margin is the ultimate goal in the surgical management of chest wall tumours [4].
A subpleural lipoma was described by Lebecque et al., underlining the rarity of occurrence [5, 6]. As described in the case, fibrolipoma is a notably rare benign chest wall tumour in a child, given the considerable size of the tumour with its dumbbell extension reaching up to the lung hilum.
Excision by a subcutaneous stealth route is an option to consider if an optimal cosmetic outcome is desired in a localized lesion [3].
In summary, fibrolipoma can present as a benign chest wall tumour in a child. Surgical excision is the treatment of choice, offering complete cure. Chest CT is helpful in planning surgical excision by delineating the relations of the lesion.