









Introduction
Regular physical activity and social interaction are crucial in maintaining cognitive functions, and decelerating age-related degenerative changes [1]. Sufficient physical activity is also important to keep conditioning and maintaining physical performance such as balance function and walking [2, 3]. Previous findings have shown that regular exercise, especially aerobic and resistance training, can attenuate cognitive impairment and dementia by modulating brain neuroplasticity in aged people [4–6]. Stimulation of cytokine factors (IL-1, TNF-α), anti-inflammatory effects, and regulation of cell insulin sensitivity are among the physiological effects of exercise [7]. Therefore, steady life and isolation evoke destructive effects on mental and physical performance by accelerating age related consequences.
Due to the pandemic outbreak of severe acute respiratory syndrome, SARS-CoV-2, the older adult population are more likely to be affected due to their vulnerability [8–10]. A weak immune system and comorbid age-related diseases such as diabetics mellitus [11], hypertension, and neurodegenerative disease are factors that endanger older individuals to be infected and increase their risk of mortality. Therefore, adherence to the World Health Organization guidelines is crucial for older adults by keeping social distance and self-quarantine. However, lower physical activity and limited social interaction imposed by quarantine can affect their mental and physical health and quality of life [8, 9, 12–14]. Evidence also revealed an increase in the experience of sarcopaenia, anxiety, and depression among older adults during long-term isolation [15]. It also has been revealed that physical performance is disrupted by the body deconditioning in these situations [16].
Recent evidence demonstrated that inactive adult women over 60 years of age are at greater risk for death, fractures, and recurrent falls than active peers of the same age [17]. The experience of cognitive and motor impairment is more prevalent among older women [18]. Most older adults, especially frail individuals, are more vulnerable to adverse health outcomes such as falls and disability [19, 20]. Therefore, their susceptibility to the complications of self-quarantine could be severe and rapid.
Considering the importance of maintaining physical activity and social participation in the mental and physical health of the older adults, self-quarantine can have a significant impact on the overall cognitive function and motor ability of this population, especially older adult women. Therefore, the present study investigates the effect of self-quarantine on the cognitive function, balance, and fall risk among older adult women.
Material and methods
Participants and study procedure
This study was conducted on 75 adult women aged over 60 years old in Tabriz, Iran in November 2019 (before the COVID-19 outbreak) and June 2020 (during self-quarantine period when COVID-19 prevention strategies were implemented) to assess their cognitive and balance functions (this study was part of a larger study to investigate the effect of neuroscience interventions on the balance and attention status of older adults). In total, 75 women were selected using the convenience sampling method from Tabriz older adult health centres (including 4 centres: Monampour, Mobin, Bakri, Parvaz, and Ibn Sina). Inclusion criteria were being 60 years old and above, being able to speak, and not having cognitive impairment [using the mini-mental state exam (MMSE) and participants’ medical history]. After selecting the participants and obtaining written informed consent, their demographic information was collected. Then, all the COVID-19 prevention protocols were observed in the second stage. Test training was held for the participants for 10 minutes.
Measuring instruments
Demographic questionnaire
The demographic questionnaire included information such as age, level of education (elementary school, diploma and university), body mass index (BMI), marital status (single/married), and physical activity (less than 30 min per week, 30–60 min per week, and more than 30 min per week).
Mini-mental state exam
The mini-mental state exam is a commonly used questionnaire, which was firstly designed and developed by Folstein et al. [21]. This 30-item tool examines the severity of cognitive impairment and cognitive changes over time in 6 dimensions, including temporal and spatial orientation, information recording, attention and calculation, the evocation of 3 words, language and its skills, skills related to three-dimensional vision, and executive functions [22]. The total scores range from 0 to 30, with lower scores indicating more severe cognitive impairment. The scores indicate 4 domains of severe cognitive impairment (mean score of 0–10), moderate cognitive impairment (mean score of 11–20), mild cognitive impairment (mean score of 21–26), and normal cognition (mean score of 27–30). Its validity and reliability in Persian language were examined and confirmed by Foroughan et al. [23]. The specificity and sensitivity of the test were obtained as 84% and 90%, respectively. The participants with scores below 21 were considered to have cognitive impairment [22].
Timed up and go test
The timed up and go test was originally developed for clinical evaluation of balance performance in the older adult population. Timed up and go is a simple screening test that is a sensitive and specific measure of probability for falls and balance among older adults. It is a quick test to conduct, without the need special equipment, and it is highly reliable and valid, providing useful outcomes related to reduced fall risk [24]. Podsiadlo et al. provided the timed version of this test, which was scored based on the time required to perform the test [25]. The validity and reliability of the test were very high, with a Cronbach’s alpha value of 0.99 and r = 0.98 in the older adult population [26]. In this test, the participants start from a sitting position on a chair and stand up. After walking for 3 m with the maximum possible speed, they turn back, walk to the chair, and sit down again. Given that the test is a timed scale, the time (sec) it takes the participants to perform this movement from standing up from the chair to sitting down on it is recorded by a chronometer [27]. Due to the movement problems of older adults and to increase the accuracy of the test, this test was repeated 3 times for each lower extremity, and then their average values were calculated for subsequent analysis.
Single leg stance test
The single leg stance test is used to assess static postural and balance control. The single leg stance test is a valuable clinical tool for monitoring neurological and musculoskeletal status as well as for managing fall risk [28]. The single leg stance test was used to evaluate the static balance performance of the participants with their eyes closed and arms on their hips. The amount of time (sec) the individual was able to stand on one limb was measured by a chronometer. The time commenced when the individual raised their foot off the floor and ended when their leg touched the ground or their supporting leg or their arms left the hips. This test evaluated the balance performance of the right and left extremities separately. The total score was obtained by calculating the average of the 3 trials [29]. This test was repeated 3 times for each lower extremity, and then their average values were calculated for subsequent analysis. We allowed a 1-min rest between successive trials.
Johns Hopkins fall risk assessment tool
The Johns Hopkins fall risk assessment tool evaluates the risk factors for falls and predicts the risk of falls in older adults. The Johns Hopkins fall risk assessment tool was developed by the Johns Hopkins Hospital in 2005 and was revised in 2007. This tool consists of 7 items, including age, fall history, elimination, medication, patient care devices, mobility, and cognition. The total score ranges from 0 to 34. The participants with scores of 14 and higher were considered to be at high fall risk [30, 31]. The validity and reliability of this tool have been assessed among older Iranian adults. The Cronbach’s alpha coefficient of the Persian version of the tool was reported to be 0.73 [32].
Ethical approval and consent to participate
This study was approved by the Ethics Committee of Tabriz University of Medical Sciences (ID number: IR.TBZMED.REC.1398.1054), and before the implementation of this research the objectives of the study were explained to participants and they were assured of the confidentiality of their individual information in the study. Written informed consent was obtained from all the study participants. All the participants were ensured about the confidentiality of their responses, identity, and the right to withdraw from the study at any stage.
Data analysis
For descriptive analysis of the data, absolute and relative frequency distribution measures, mean, and standard deviation were applied. For inferential analysis of the data, Shapiro-Wilk statistical test was used to examine the normality of the data, and paired t-test (or Wilcoxon test) was employed to compare the baseline and quarantine conditions. Moreover, the data were analysed using SPSS 26.0, and the figures were plotted by G*Power 3.1.9.6 and GraphPad prism 9.1. The significance level of p < 0.05 was considered in all the analyses.
Results
The mean age of the participants was 62.9 ±3.74 years, and most of the participants were married. The mean BMIs of the participants in the baseline and quarantine conditions were 24.46 ±5.85 and 27.68 ±4.35, respectively (Table 1).
Table 1
Descriptive data of the participants
The results comparing the variables at baseline and quarantine conditions are presented in Table 2 and Figure 1. The results indicated a significant difference in the mean cognitive scores at baseline and quarantine conditions (p < 0.001), so that the mean cognitive score in quarantine was significantly lower than that at the baseline. The mean fall risk score in quarantine was significantly higher than that at the baseline (p < 0.001). Also, no significant difference was observed in the mean static balance between the baseline and quarantine conditions. The mean dynamic balance in quarantine was significantly higher than that at the baseline (p < 0.001).
Fig. 1
Comparing the mean cognitive status, fall risk, static balance, and dynamic balance in baseline and quarantine conditions
MMSE – mini-mental state exam, SLS – single leg stance, TUG – timed up and go
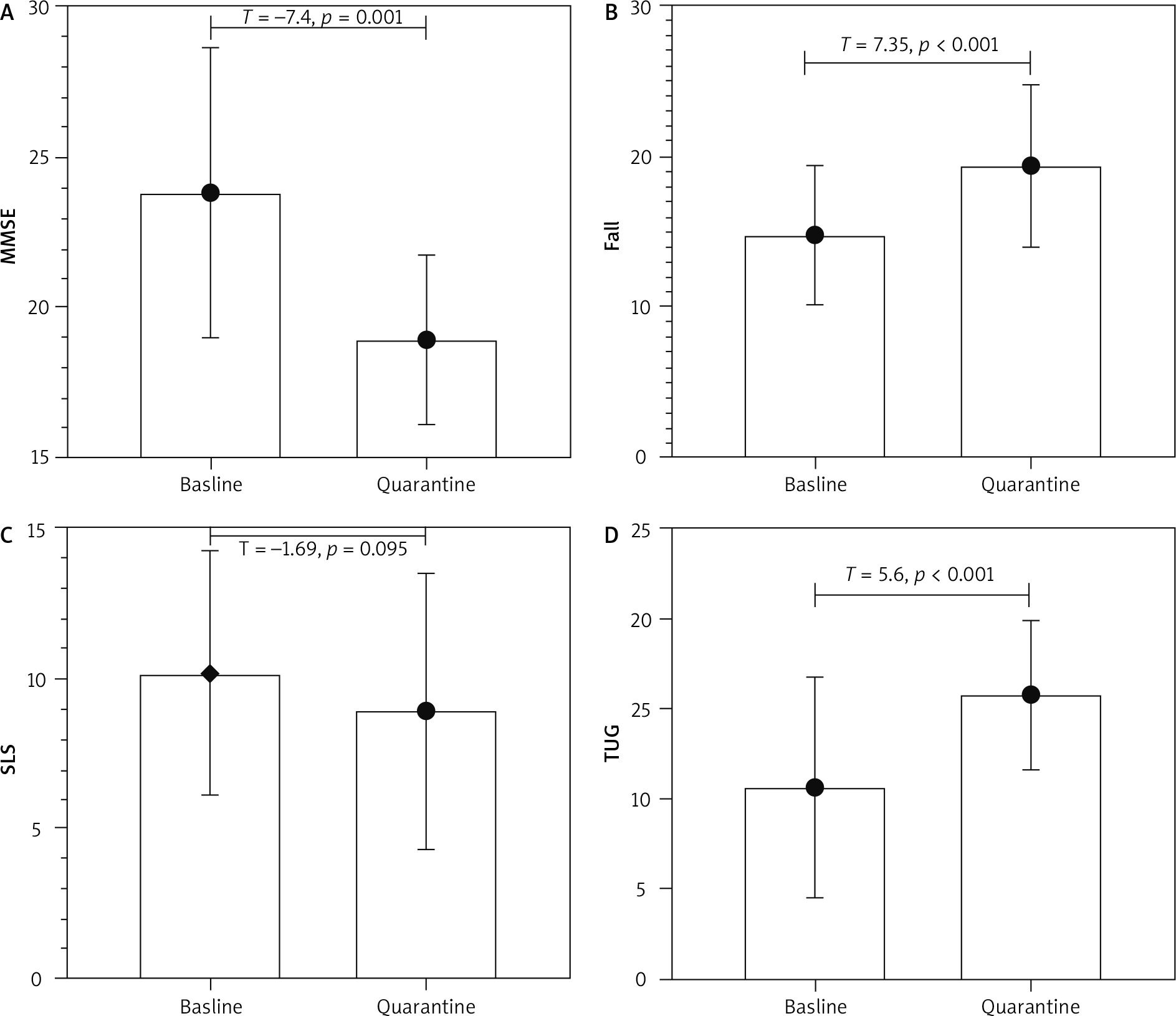
Table 2
Comparing the mean values of study variables in baseline and quarantine conditions using the Wilcoxon test
Implication for practice
Because older adults will lose their cognitive function and balance because of having fewer social activities, policymakers should legislate rules to increase the activity of older adults, and health systems should prepare programs to increase the activities of the older adult population in the community. On the another hand, to prevent the loss of cognitive and balance abilities among older adults in the COVID-19 era, due to spending more time at home, it is suggested that programs are developed to improve the cognitive function and balance of older adults.
Limited social activities for older adults who spend most of their time at home reduces their cognitive function and balance. Therefore, policy makers should design programs to increase the participation of older adults in society. In this regard, the health system should also consider programs for the active participation of the older adult population in the community, in the planning process related to this segment of society. To prevent the decline in the cognitive and balance abilities of older adults in the time of COVID-19 it is suggested that programs be set up so that older adults can interact with each other through social media or through WhatsApp groups, and a series of exercises and activities from Predict the health system side for these at home.
Discussion
This study investigated the cognitive and balance performance of the old women who were in quarantine during the breakout of the COVID-19 pandemic, and the findings indicated that the balance and cognitive abilities were disrupted after 7 months of self-quarantine at home and the participants were at greater risk of fall. Female gender has been shown to be an effective factor in attenuating cognitive abilities in developing countries such as Iran, suggesting that older adult women are at higher risk of physical and cognitive impairment than older adult men [18].
According to the results, older adult women’s cognitive function was significantly impaired after 7 months of quarantine. Consistent with the present study, Kouzuki et al. examined the effect of quarantine associated with COVID-19 by conducting phone interviews with the caregivers of 31 older people with mild cognitive impairment (MCI) and found that cognitive function declined in 41% of the participants [33]. Furthermore, investigations have shown that self-quarantine during the COVID-19 pandemic caused social isolation and reduced individual activities, and increased the risk of cognitive decline in the older adults [34, 35]. These studies suggest that cognitive impairment in older adults may be associated with depression and anxiety in critical situations as well as with reduced social participation [36].
Few studies have examined the impact of self-quarantine on cognitive outcomes, especially among the older adults. The results of these studies have been relatively consistent with the findings of the present work. They have reported a correlation between social isolation and depression, anxiety, and decline in cognitive performance such as executive function among older adults. In addition, these studies reported a high frequency of diseases such as sleep disorders, cardiovascular deconditioning, and immunodeficiency disorders associated with the social isolation of older adults [37]. Investigations examining the impact of natural disasters on older adults have also revealed impairment of their cognitive functions in critical situations [38].
Cognitive impairment associated with self-quarantine in the present study was among the psychological outcomes of the COVID-19 pandemic, which may be caused by reduced social participation and the resulting emotional problems [39]. Recent studies have confirmed the determinant effect of social isolation on cognitive decline in domains such as executive function and memory [40]. Some studies have shown that the COVID-19 pandemic has no significant effect on the mental health status of the older adults [41–43]. However, it should be noted that these studies have been conducted at the beginning of the COVID-19 outbreak and probably have not considered a sufficient period to study the effects of self-quarantine on the performance of the older adults. Cognitive decline is a part of physiological aging and is not considered a debilitating disease [44, 45]. It can be influenced by factors such as physical activity, participation in motivational activities, and social networks [46].
In line with the results of the present study, some studies have introduced social participation as a stimulus to increase physical activity levels [47–49]. The results have suggested that physical dysfunction in older adults can be explained by decreased social interactions. In support of this hypothesis, studies have shown that the COVID-19 outbreak reduced the social engagement [50]), physical activity [50], and mental health of older adults and led to depression, anxiety, and consequently to cognitive impairment and increased social isolation [11].
Declined balance function and increased risk of falling among older adults in quarantine conditions can be explained by physiological and biomechanical changes due to prolonged stay at home [11]. Decreased physical activity can lead to obesity and overweight [51]. The present study shows that BMI increased during quarantine. Increasing body mass can disrupt the efficiency of balance responses of the musculoskeletal system and brain centres by altering the parameters related to maintaining balance such as the centre of pressure and fluctuations of the body centre of gravity and weaken all control strategies in older adults [52]. Studies have revealed that reduced sun exposure can lead to mood disorders and changes in endocrine gland secretions [53]. Changes in vitamin D synthesis due to reduced sun exposure can also weaken the immune system and affect cognitive and balance functions [53]. As a result, infections occur more often, and the risk of falls increases [53, 54]. Tramontana et al. found a direct correlation between vitamin D synthesis during the COVID-19 pandemic and musculoskeletal changes in older adults [55]. Studies have reported a direct correlation between vitamin D deficiency, impaired balance, and increased fall risk in older adults [56]. Moreover, quarantining older adults in the enclosed space of the house can be regarded as one of the causes of developing balance disorders. Studies have shown that quarantining older adults at home increases the risk of falls in people with balance and movement disorders such as Parkinson’s disease and dementia [57]. Finally, reduced access to physical activity, fear of falling, and decreased motivation due to the psychological burden of the pandemic can lead to a sedentary lifestyle [51] and thus exacerbate mental and physical impairment in older adults [58]. Accordingly, older people are advised to regularly exercise at home, increase mobility, use balance and cognitive exercises in order to increase conditioning, and reduce balance disorders in isolation conditions [59].
Because this was a cross-sectional study, a causal relationship could not be established between the variables. Given that the studied sample was selected from the older adult-friendly centres, this may not be considered as representative of the whole community. All the studied variables were based on self-reports and thus may be prone to reporting bias. The data were collected from one city in Iran. Therefore, the results may not be generalizable to different cultural and societal settings. Cognitive functions were assessed using MMSE, which has some significant shortcomings. This scale overlooks age, education, and cultural and socioeconomic variables. It is also well-known for the “ceiling effect” when used for poorly educated people and for the “floor effect” for those with higher education [60]. Moreover, the mean MMSE decline was applied to the whole sample, which might not account for individual variabilities. Nevertheless, the MMSE is brief, widely accepted, easily administered in the clinical setting, and is the most commonly used cognitive disorder screening tool globally; it has been translated into different languages and standardized in different cultures. Finally, although our study was not designed longitudinally, it evaluated the variables twice, i.e. pre-quarantine and post-quarantine, which made a direct comparison of the studied criteria. As a result, it can minimize the problems associated with changes. Therefore, our findings regarding the cognitive status, risk of falling, and impaired balance could highlight the effects of self-quarantine during the COVID-19 period.
Conclusions
This study showed that self-quarantine can reduce the cognitive performance of older adults and increase the fall risk in this group by disrupting balance functions. It implies that the reduced social participation and psychological burden resulting from the COVID-19 pandemic were among the causes of cognitive changes. Also, decreased physical activity due to staying at home as well as reduced personal motivations and social activities were effective factors in balance changes in this population. It is recommended that the consequences of prolonged self-quarantine due to COVID-19 on the health and performance of the older adults is further investigated in future studies.