






Large secundum atrial septal defects (ASD) with deficient or absent rim(s) remain a challenge for percutaneous closure and may require modified implantation techniques for successful device delivery [1]. Deployment from the right upper pulmonary vein or balloon-assisted positioning are effective methods of device implantation in challenging defects [2, 3]. However, in some patients even these techniques fail, and repeat attempts of device positioning or significant device oversizing may lead to complications [4]. We present a combination of modified implantation techniques for closure of a large secundum atrial septal defect with deficient rims.
During a routine examination of an asymptomatic, 13-year-old girl regularly practicing sports (59 kg) a murmur over the heart was heard. Transthoracic echocardiography showed a large secundum atrial septal defect with deficient aortic rim, right ventricular dilation, and moderate tricuspid regurgitation with a pressure gradient of 45 mm Hg.
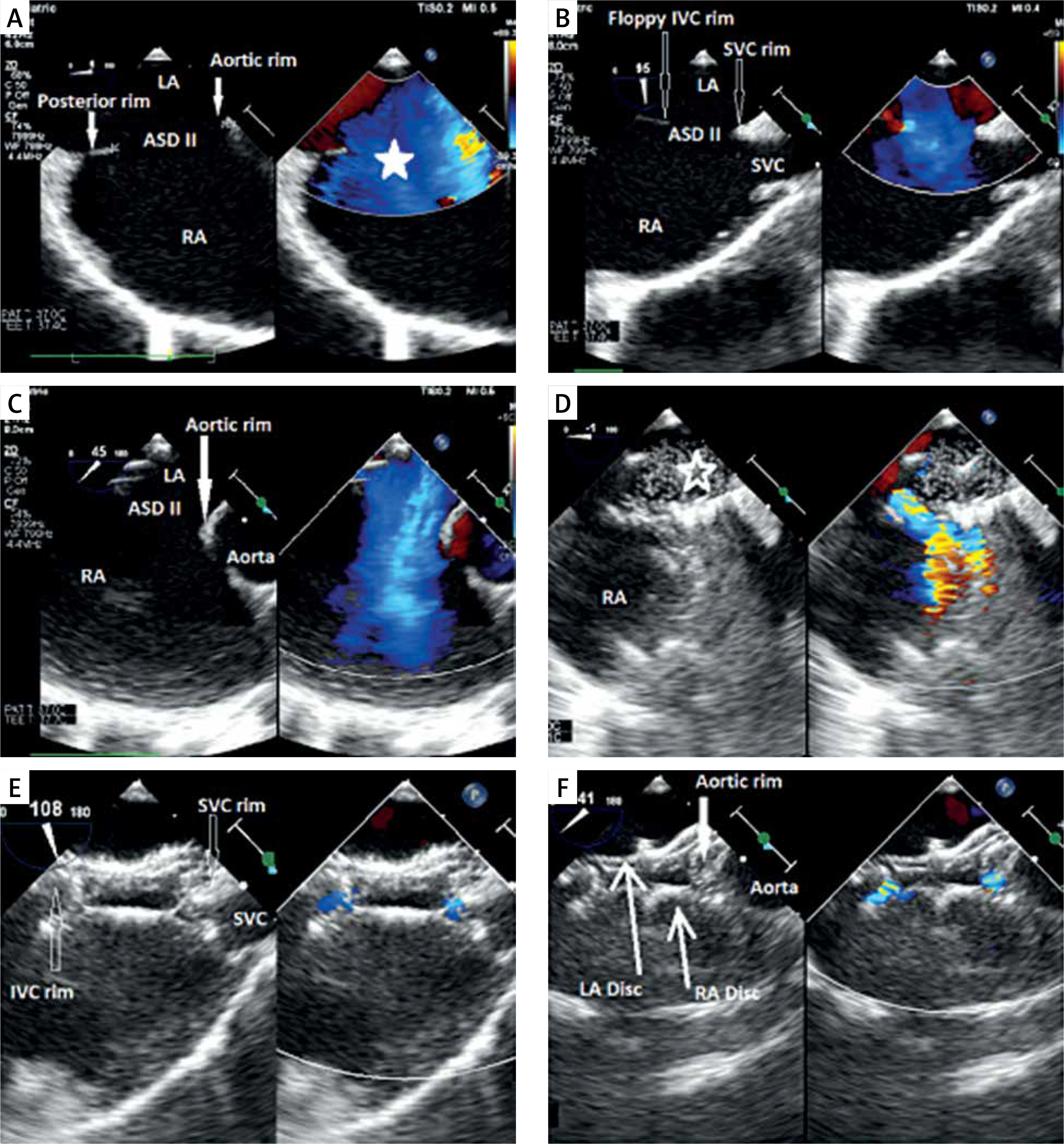
Transoesophageal echocardiography (Figure 1), performed under general anaesthesia, confirmed a large secundum atrial septal defect measuring up to 27 mm with deficient aortic rim, floppy inferior vena cava rim, and a short superior vena cava rim.
Figure 1
Transoesophageal images of device closure of a large secundum atrial septal defect with deficient superior vena cava. A – Four-chamber view (zoom); on the left side: secundum atrial septal defect in the middle part of the septum, dilated right atrium. Good visualization of the present posterior rim and deficient aortic rim; on the right side: TEE with colour Doppler showing a very large atrial septal defect with left-to-right shunt (white star). B – Bicaval view presenting a short superior vena cava rim and thin and floppy inferior vena cava rim. C – Short-axis view focused on the aortic valve showing lack of the aortic rim. D – Sizing balloon catheter inflated across the defect (empty white star) during simultaneous device deployment from the right upper pulmonary vein. E – Final result after release of the device; bicaval view with colour Doppler compare TEE showing typical device conformation with small residual leaks and unobstructed flow from the superior vena cava. F – Final result after release of the device: short-axis view with colour Doppler compare presenting the occluder well positioned on the aorta with small residual flow
SVC – superior vena cava, IVC – inferior vena cava, Ao – aortic valve, LA – left atrium, RA – right atrium, ASD II – secundum atrial septal defect.
Subsequently, right and left heart catheterization was performed. In view of favourable haemodynamic measurements – the mean pulmonary artery pressure of 15 mm Hg, indexed pulmonary vascular resistance of 1.0 Wood Units, and pulmonary-to-systemic flow ratio of 3.2 : 1 – the decision was made to attempt defect closure.
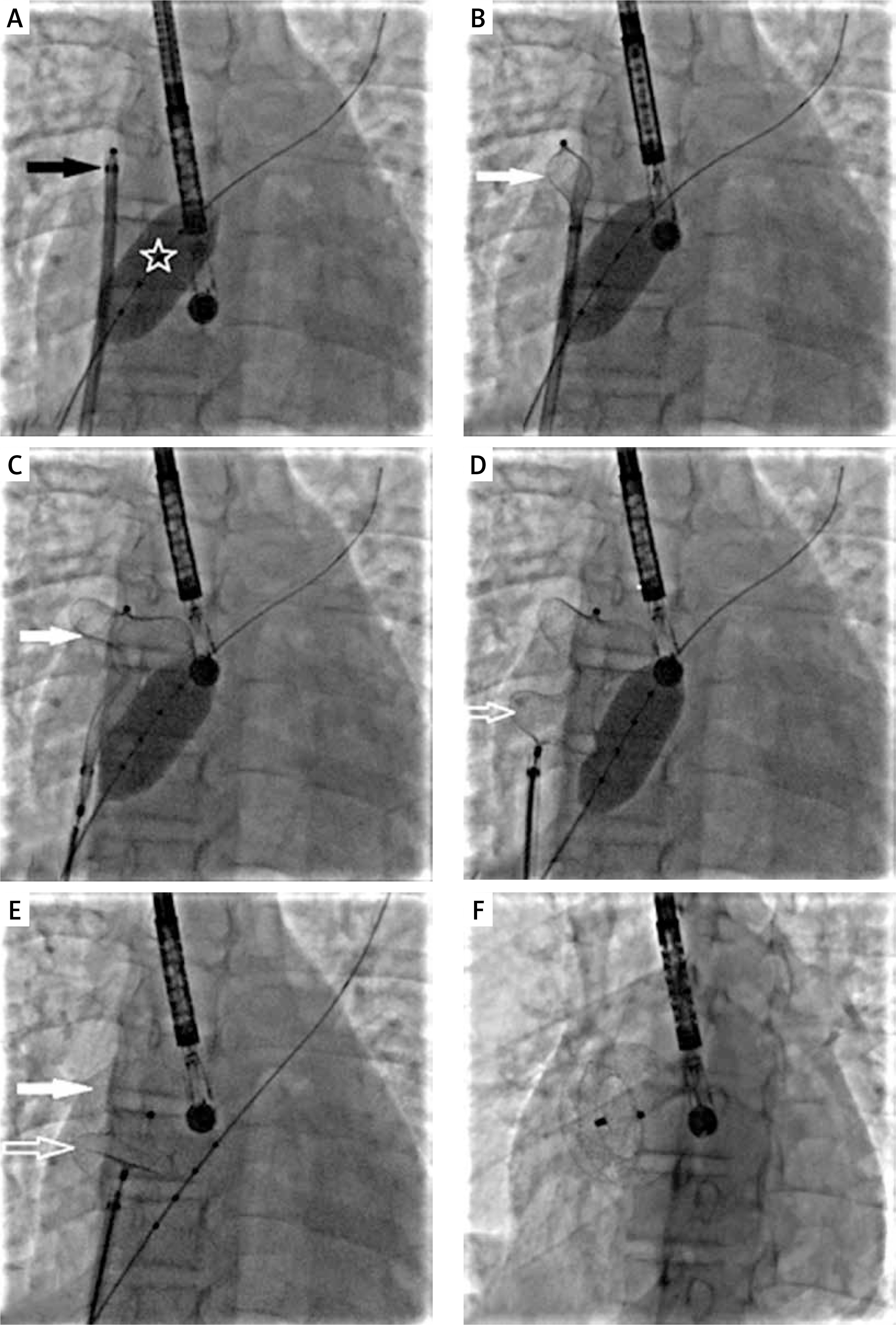
A 30-mm Amplatzer Septal Occluder (Abbott) mounted on a classic delivery cable was introduced via a standard 10 Fr TorqueVue sheath (Abbott); however, due to the large size of the defect and deficient rims, a stable implant position was not obtained. The left atrial disc slipped across the defect to the right atrium. Through an additional femoral vascular access, a 25-mm diagnostic sizing balloon catheter (NuMed) was inserted into the defect. Next, the balloon was simultaneously inflated (Figure 2 A) and the left atrial disc was deployed starting in the right upper pulmonary vein (Figures 2 B, C) followed by deployment of the right atrial disc (Figures 2 C, D). With stable device position the balloon was deflated (Figures 2 E) and gently withdrawn. After echocardiographic confirmation of the optimal position of the occluder and unobstructed flow from the superior vena cava, the device was released (Figure 2 F). With a combination of 2 modified techniques the device was deployed successfully in the first attempt.
Figure 2
Percutaneous large secundum atrial septal defect closure with combination of modified techniques. A – A sizing balloon (white star) is inflated with the long sheath and the occluder (black star) ready for deployment in the right upper pulmonary vein. B – The left atrial disc (white arrow) being deployed in the right upper pulmonary vein. C – The left atrial disc (white arrow) fully deployed with the sizing balloon inflated. D – The right atrial disc (white empty arrow) deployed with sizing balloon inflated. E – Gradual deflation of the sizing balloon after both discs have been deployed and progressive conformation of the discs (white arrows) as the balloon is completely deflated. F – Final position of the device after release
Transthoracic echocardiography performed on the following day showed stable implant position without colliding with intracardiac structures. Further hospital stay and follow-up were uneventful. The device remained stable in 6 months of follow-up without residual flow. The tricuspid insufficiency diminished to mild just 1 month after implantation, with simultaneous gradient reduction to 17 mm Hg.
Percutaneous device closure of secundum atrial septal defects is routine clinical practice [5]. Occasionally, large size of the defect, deficient rim(s), or floppy septum warrant modified implantation techniques, which also come with some disadvantages [2, 3]. For instance, the balloon-assisted technique requires additional vascular access, and disc deployment in the pulmonary vein creates a risk of vein perforation. Furthermore, multiple attempts of device deployment may increase the likelihood of damaging the pulmonary vein or atrial wall [4].
A recently introduced novel delivery system, providing major flexibility and tension reduction, enables more predictable and efficient device closure of large atrial septal defects [6]. In cases when conventional technique and improved delivery system prove insufficient, a combination of modified techniques, such as balloon assistance and right upper pulmonary vein approach, enable successful device delivery even in a single attempt and exclude the need for significant device upsizing.