






Coronary slow flow (CSF) is a phenomenon characterized by delayed distal coronary inflow of contrast, accompanied by the absence of significant atherosclerotic changes in the epicardial arteries. CSF is defined as corrected TIMI frame count (CTFC) > 27, which is the number of cine frames required for the contrast run-off from the coronary artery [1]. CSF represents one of the endotypes of ischemia and no obstructive coronary arteries (INOCA) and suggests microvascular angina (MVA), according to the EAPCI Expert Consensus [2]. Here, we describe a patient with chest pain due to MVA, which resolved after initiation of treatment with calcium channel blockers (CCB).
A 67-year-old woman with exertional angina (CCS class III), arterial hypertension and hypercholesterolemia was admitted to the cardiology department for diagnostic work-up. Physical examination, basic laboratory tests, resting electrocardiogram (ECG) and transthoracic echocardiography showed no significant abnormalities. During ECG on exertion, the patient experienced chest pain with concomitant ST-segment depression in leads II, III, aVF, and V4-V6. Coronary angiography performed 3 months earlier had showed no significant atherosclerosis in the epicardial coronary arteries (Figures 1 A, B). An initial diagnosis of INOCA was made.
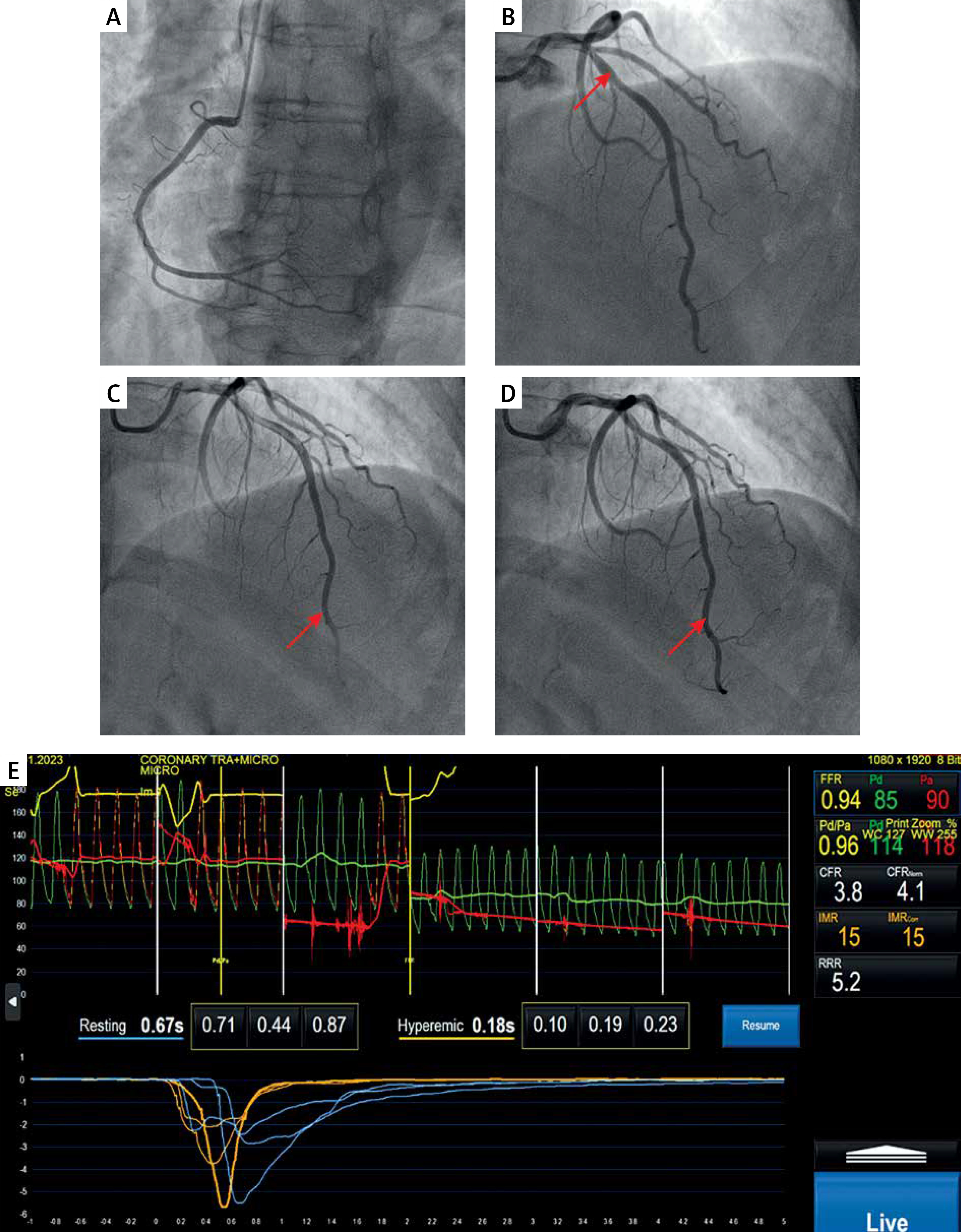
Figure 1
Coronary angiography showing normal right coronary artery (A) and 20–30% stenosis in the mid segment of the left anterior descending artery (B, red arrow). Coronary slow-flow phenomenon was induced after administration of 2 mg of acetylcholine (C) and resolved after intracoronary nitroglycerine injection (D). Evaluation of coronary microvascular function using the CoroFlow software (Coroventis, Uppsala, Sweden) and PressureWire X (Abbott Laboratories, Illinois, United States) with the pressure-temperature sensor (E) showed normal values of fractional flow reserve, coronary flow reserve and index of microcirculatory resistance (FFR = 0.94; CFR = 3.8; IMR = 15, respectively)
To expand the diagnostics towards MVA, coronary microvascular function was assessed using CoroFlow software and PressureWire X. A pressure-temperature sensor was applied in the left anterior descending artery (LAD) territory and the acetylcholine (ACh) provocation test was performed. Following intracoronary administration of 200 mg of nitroglycerin, fractional flow reserve (FFR), coronary flow reserve and index of microcirculatory resistance were measured in real time in the LAD territory at rest and during hyperemia using thermodilution. Hyperemia was achieved by an intravenous infusion of adenosine (140 μg/kg/min). Thermodilution was performed by intracoronary injection of 3 ml of saline. All values were within the normal range (FFR = 0.94; CFR = 3.8; IMR = 15, respectively). Subsequently, ACh was prepared according to the standardized protocol (doses of 2 μg, 20 μg, 100 μg and 200 μg). Already after intracoronary administration of the smallest, 2 μg ACh dose, the patient reported chest pain, which was accompanied by ST-segment depression in leads II and III and CSF in the coronary angiography, without epicardial LAD spasm (Figure 1 C). Another 200 mg of nitroglycerin was administered intracoronary, leading to resolution of anginal pain (Figure 1 D). The CTFC values at baseline, after ACh and nitroglycerin administration were 16.5, 28.2 and 16.5 frames, respectively. A diagnosis of MVA (microcirculation spasm) was made [3]. A CCB (amlodipine) was started and previously used treatment of comorbidities was continued (acetylsalicylic acid, perindopril, indapamide and atorvastatin), leading to anginal symptom alleviation during 2-month follow-up in the outpatient clinic.
Clinical criteria for suspecting MVA include signs and symptoms of INOCA (< 50% diameter reduction or FFR > 0.80) and evidence of impaired coronary microvascular function. Identification of the MVA mechanism by invasive coronary function testing is critical to stratify medical therapy, with β-blockers, angiotensin-converting enzyme inhibitors and statins indicated in case of impaired microcirculatory conductance, and CCBs and long-acting nitrates in patients with epicardial or microvascular spasm [4]. Such tailored therapy was shown to decrease angina burden and improve quality-of-life score in patients with INOCA included in the CorMicA Trial [5]. Although the diagnostic usefulness of CSF has been questioned in some studies [6], the recent Expert Consensus suggested that CSF should be considered in MVA, especially if combined with anginal symptoms and ischemic ECG alterations, suggesting microvascular spasm [2].