
Dear Editor,
Central airway obstruction (CAO) caused by an intraluminal mass is a life-threatening situation frequently causing respiratory decompensation. Therefore, initial management in CAO is based on the etiology, patient symptoms, prognosis, and degree of obstruction. If a critical obstruction is present, it is essential to successfully debulk the tumor mass in order to provide significant symptom relief to improve quality of life [1]. Herein, we present a case of pre-emptive veno-venous extracorporeal membrane oxygenation (VV-ECMO) to facilitate an emergency resection with rigid bronchoscopy of an intraluminal tracheal tumor with Myer-Cotton grade III stenosis located in the lower third of the trachea [2]. Written consent was obtained from the patient for this presentation.
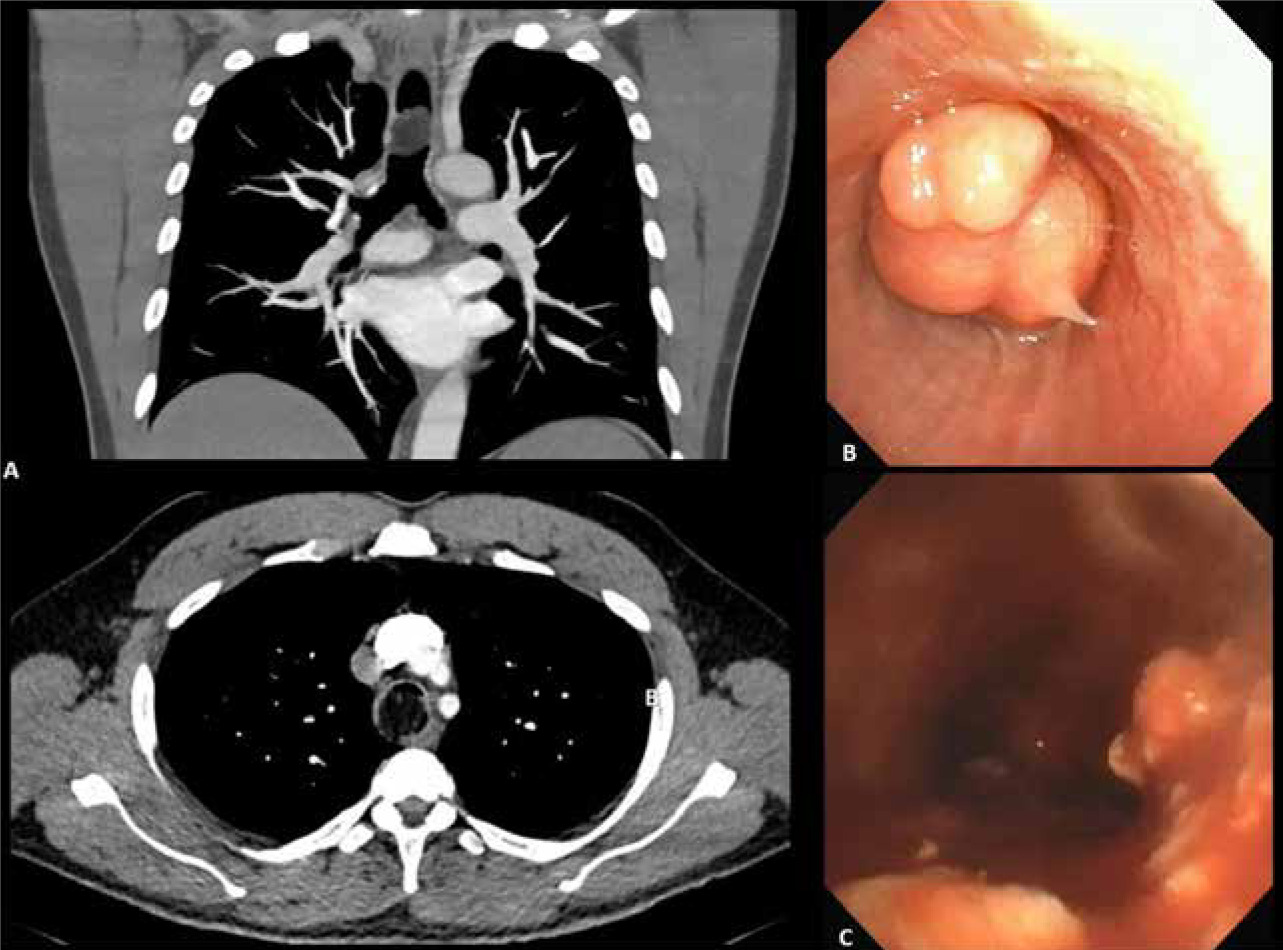
A 44-year-old man had two episodes of shortness of breath, anxiety, and a short period of losing consciousness. He was recently diagnosed with asthma with no improvement from salbutamol and montelukast. He experienced dyspnea and wheezing while supine and upon exertion and was sleeping in the right lateral decubitus position. A chest computed tomography (CT) scan showed a large fat density mass with 90% tracheal obstruction, 2.5 cm above the main carina (Figu- re 1A). The patient was transferred to our center for urgent management. On arrival, he had severe respiratory distress and was brought into the ope-rating room for emergent tumor resection.
Considering the location and size of the tracheal mass, we established VV-ECMO pre-emptively before the induction of general anesthesia. The baseline pulse oximetry (SpO2) was 96%, oxygen (6 L min–1) was delivered through a face mask, and then the patient was sedated with low- dose midazolam, fentanyl, and propofol infusion while maintaining spontaneous ventilation. He was anticoagulated with 5000 U of intravenous (IV) heparin, which achieved an activated clotting time (ACT) of 260 seconds. When the ACT value was < 160 s, additional unfractionated heparin bolus doses (10–40 UI kg–1) were administered according to our institutional protocol. The patient underwent right femoral (RFV) and right internal jugular (RIJV) venipuncture with ultra-sound guidance. Then, cannulation was performed with a 24 Fr inflow cannula placed in the inferior vena cava (drainage) and RIJV cannulation with a 21 Fr outflow cannula (oxygenated blood return) placed in the superior vena cava, guided by anatomical landmarks. The flow was started at 5.13 L min–1 (full calculated flow for a cardiac index of 2.4 was 5.2 L min–1), then maintained at 5–5.5 L min–1 with 100% FiO2 and sweep gas at 2–3 L min–1, SpO2 increased to 99%, and general anesthesia without muscle relaxation was induced. A laryngeal mask airway (LMA) was placed under spontaneous ventilation. Then, rocuronium was given, protective lung ventilation started with adequate chest excursion, and end-tidal CO2 was obtained, meaning the patient could be ventilated with positive pressure ventilation. While on ECMO, general anesthesia was maintained with propofol, remifentanil, and rocuronium, and depth of anesthesia was monitored with the patient state index (Sedline Inc., San Diego, CA, USA). SpO2 and arterial blood gas testing confirmed the adequacy of gas exchange with ECMO. With oxygenation and ventilation ensured by VV-ECMO, rigid bronchoscopy was performed (Figure 1B); high-frequency jet ventilation could be performed if necessary. The mass was challenging to resect as it was mobile and elastic; an electrocautery snare was used to debulk it (Figure 1C).
FIGURE 1
Perioperative tracheal tumour resection. A) Preoperative chest computed tomography scan (coronal and axial views) with tumour obstructing the distal trachea. B) Rigid bronchoscopy image showing an endotracheal tumour obstructing most of the tracheal lumen. C) Postoperative findings with tracheal patency
One hour after the start of surgery, SpO2 decreased to 90%, partial oxygen pressure (pO2) decreased to 61 mmHg, and ECMO flows increased to 6 L min–1. ECMO circuit and adequate membrane oxygenation were verified. As this was an emergency operation in a life-threatening situation, we did not have transesophageal echocardiography or fluoroscopy available to confirm the position of the cannulas. We suspected a recirculation event and withdrew the inflow cannula 5 cm to re-establish adequate oxygenation and ventilation. Rigid bronchoscopy was restarted, and 60% patency of the airway was secured. Due to airway edema despite a high dose of steroids, we elected to keep the patient intubated. The tube was positioned with the balloon over the resection site to obtain hemostasis and the patient was decannulated at the end of the procedure (2.5 hours). The following day, under bronchoscopic view, the tube was gradually retracted, the remaining tumor was visualized with no active bleeding, and the patient was extubated and recovered in the intensive care unit (ICU). Four days after surgery, he suffered a deep vein thrombosis in his left leg and a pulmonary embolism. Anticoagulation was started, and he was discharged 13 days after surgery.
Surgical pathology examination revealed a diagnosis of lipoma. The thrombosis clinic is following him up, and the plan is to perform a laser debridement to complete the resection after his anticoagulation is discontinued.
Primary tracheal tumors are uncommon; the incidence is about 0.1 in every 100 000 persons per year, corresponding to 0.02 to 0.04% of all malignant tumors (fewer than 0.2% of tumors). Benign CAO is more frequently secondary to tracheal intubation, inflammatory, or infectious disease and is a rare condition. Histologically, benign endobronchial tumors can present as squamous papilloma, pleomorphic adenoma, fibrous histiocytoma, leiomyoma, chondroma, lipoma, or vascular malformations, among others [3, 4]. Benign and malign CAO have a similar clinical presentation and cause signs and symptoms of airway obstruction (dyspnea, shortness of breath, wheezing, and stridor); symptoms typically do not manifest until the tracheal narrowing is less than 8 mm [5] or until they occlude more than 30% of the luminal diameter [6]. Our patient’s presentation was typical for this group; many patients are often misdiagnosed with asthma or chronic obstructive pulmonary disease, and surgical resection requires an experienced multidisciplinary team (thoracic surgeon, anesthesiologist, radiologist, intensive care unit, nurse, and perfusionist) [7].
The airway management, in this case, is challenging throughout the perioperative period as there is a high risk of inability to ventilate or having air-trapping with positive pressure ventilation. Furthermore, for tumor resection, rigid bronchoscopy requires total intravenous anesthesia (usually with propofol and remifentanil) and deep muscle relaxation [8]. Therefore, before the start of the case, different plans were discussed in a stepwise order: VV-ECMO (plan A), LMA (plan B), and high-frequency jet ventilation (plan C). VV-ECMO was previously used as a bridge to support definite airway management in cases with severe airway obstruction; it was initiated in the ICU prior to surgery, and subsequent weaning and decannulation were also performed in the ICU [9]. Also, this technique has been used as a bridge to tracheostomy [10], carinal resection [11, 12], stent implantation [13, 14], extrinsic airway compression in an anterior mediastinal mass [15], thyroid cancer [16] or for elective endotracheal tumor resection [7, 17]. Because of the nearly distal obstructing tumor, previous syncope and signs of imminent respiratory failure in our patient, awake VV-ECMO was considered to be the safest course of action.
The Canadian Airway Focus Group states that when all four airway mana-gement strategies (facemask ventilation, supraglottic airway, tracheal intubation and front of neck airway access) are anticipated to fail, awake VV-ECMO might be a safer option to sustain oxygenation [18]. Malpas et al. [19] performed a systematic review on the use of ECMO as an elective procedure prior to airway intervention; the authors acknowledged that ECMO could have provided adequate oxygenation for patients with CAO without any major complications. However, in our case, ECMO cannulation could also be an option to ensure adequate oxygenation in emergency environments.
Although ECMO can be a life-saving intervention, it should be always considered when the bene-fits outweigh the potential risks and complications [20, 21]. In VV-ECMO, only a portion of the venous return is directed to the circuit, oxygenated and returned to the right atrium, where it mixes with the remainder of the venous return. Therefore, there is a risk of shunt and hypoxemia in cases where the ECMO flow is less than the cardiac output. CO2 removal also has to be adjusted to avoid hyper/hypocarbia. There is also a risk of cannula insertion difficulties, thrombotic events, bleeding, sepsis and neurological events [5, 7, 9, 13, 22]. Insertion could be particularly difficult if the patient is unable to lie flat. Wu et al. [17] reported a 91.6% ECMO survival rate and the following complications: foot ischemia, massive airway bleeding, vein rupture and hematoma, arteriovenous fistula and neuropraxia of the cannulation site.
A recirculation event refers to post-oxygenator blood returning to the inflow cannula. It decreases the delivery of oxygenated blood to the patient, causing hypoxemia. It is more common with single-lumen dual cannulation and should be suspected with a paradoxical decrease in systemic saturation with increasing VV-ECMO flow [22]. In our case, the urgency of the procedure precluded us from confirming the positioning of the cannula; however, to avoid recirculation, it is recommended to perform it with either transesophageal echocardiography or fluoroscopy [22]. Echocardiographic evaluation is recommended not only to confirm cannula positioning but also to identify other complications such as cannula malfunction, cardiac filling, retroperitoneal hematoma, vascular damage, cardiac function or tamponade among other complications related to ECMO [23].
In summary, urgent VV-ECMO can be an alternative for managing CAO in patients with critical symptoms for therapeutic interventions or as a bridge to support the patient until the CAO is resolved. Experience with ECMO in these cases is limited to case reports and series. This requires significant institutional experience, resources, and a multidisciplinary team.