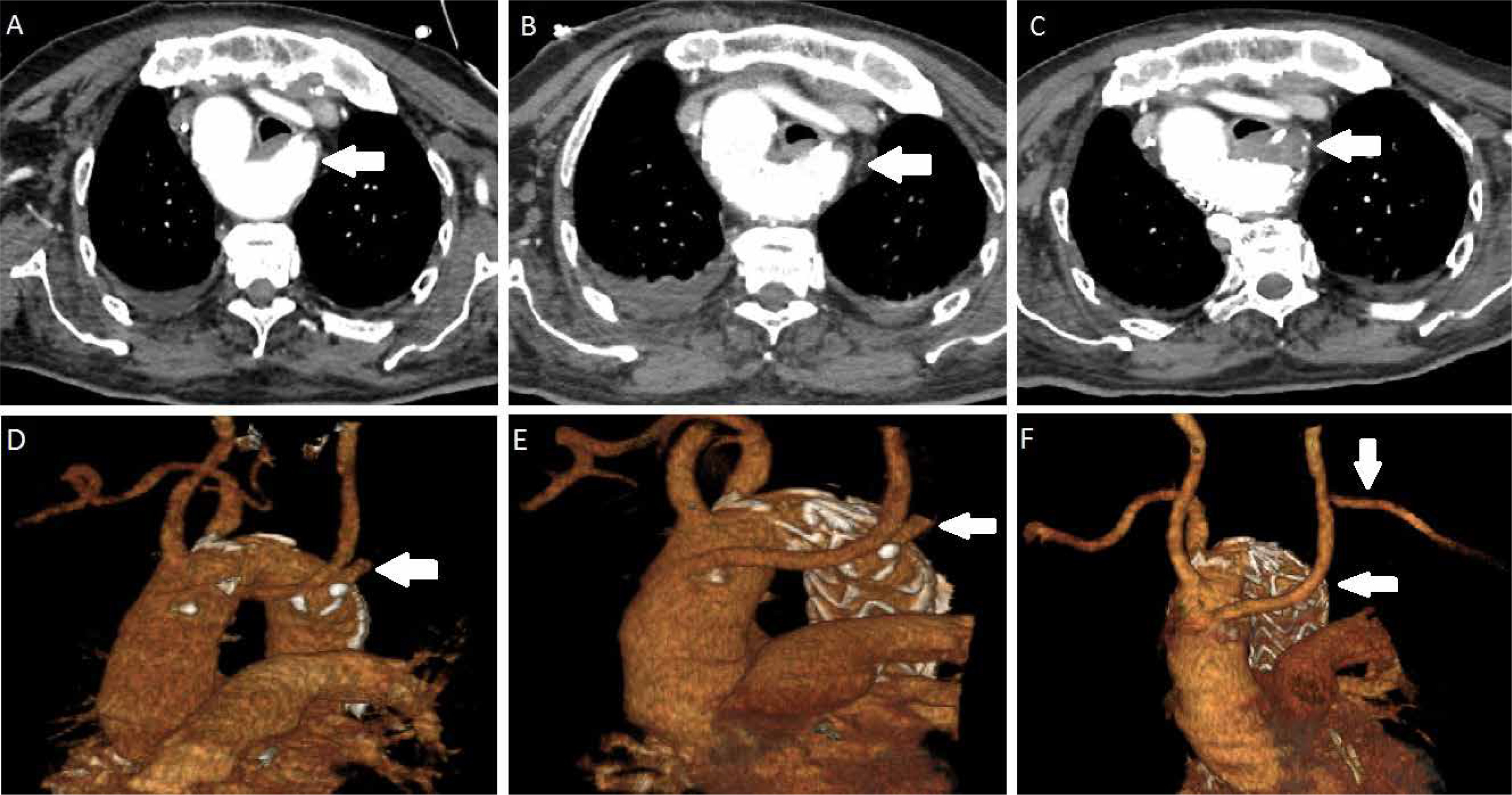
Right-sided aortic arch accompanying aberrant left subclavian artery is mostly asymptomatic and incidentally detected. Guidelines or surgical indications for Kommerell’s diverticulum have not been established because of the rareness of the anomaly. Ota et al. [1] recommend treating patients with the diameter of Kommerell’s diverticulum more than 50 mm in patients who had symptoms associated with Kommerell’s diverticulum. Czerny et al. [2] stated that aberrant subclavian arteries ≥ 3 cm in diameter and Kommerell’s diverticula with a diameter ≥ 5.5 and in addition symptomatic patients should be treated. Symptoms including dysphagia, respiratory failure, or chest pain can be present in 5% of patients. Treatments options include open surgery via sternotomy or thoracotomy under deep hypothermic circulatory and endovascular and hybrid surgery [3]. An 84-year-old man who presented with pneumonia due to compression of the trachea was admitted to our hospital. Computed tomography revealed right-sided aortic arch and the left subclavian artery arose from the descending aorta in a Kommerell’s diverticulum. The right-sided descending aorta had a maximum diameter of 45 mm and the diverticulum had a 25 mm diameter. He was intubated in the emergency service due to severe dyspnea and appropriate antibiotic therapy was administered. After informed consent had been taken from the patient’s family, a tracheostomy was performed 2 weeks after intubation. Due to compression symptoms of Kommerell’s diverticulum, the first stage was performed via a subclavian artery to carotid artery transposition and the second stage was performed via thoracic endovascular repair (TEVAR) with 40 × 40 × 150 mm Valiant Captivia (Medtronic, Santa Rosa, Calif) endograft. Postoperative computed tomography showed complete exclusion of the diverticulum and no endoleaks (Figures 1 A–F). He was removed from the ventilator 2 weeks later and discharged at 1 month postoperatively. Six months later he was doing well without dyspnea and endoleak. Here, we report a case of successful hybrid treatment and resolution of a Kommerell’s diverticulum.
Journals
Advances in Dermatology and Allergology/Postępy Dermatologii i Alergologii
Advances in Interventional Cardiology/Postępy w Kardiologii Interwencyjnej
Anaesthesiology Intensive Therapy
Archives of Medical Science
Biology of Sport
Central European Journal of Immunology
Folia Neuropathologica
Forum Ortodontyczne / Orthodontic Forum
Journal of Contemporary Brachytherapy
Pediatric Endocrinology Diabetes and Metabolism
Pielęgniarstwo Chirurgiczne i Angiologiczne/Surgical and Vascular Nursing
Polish Journal of Pathology
Prenatal Cardiology