








Introduction
Breast cancer is one of the most common cancers in women. The group most at risk of developing it are those aged 50-69 years. Importantly, this type of cancer also occurs in men (1% of all cases) [1]. The latest guidelines from the National Comprehensive Cancer Network define breast cancer by meeting any of the following criteria in the absence of metastases: tumor greater than 5 cm in size with regional lymphadenopathy (N1-3), tumor of any size with direct extension to the chest or skin, or both (including ulceration or satellite nodules), and the presence of regional lymphadenopathy regardless of tumor stage [2]. There is no single method of treatment for cancer; combined treatment is used – radiotherapy, chemotherapy and surgery [3].
Surgical treatment is the primary treatment for breast cancer including both diagnostic procedures and radical treatment, breast-conserving surgeries, breast reconstruction procedures and surgeries to alleviate the symptoms of the disease. Surgical treatment, while providing the highest chance of cure, also creates the possibility of complications not directly related to the course of the disease but resulting from the intervention. Complications may occur during, immediately after surgery or many years after surgical treatment [4].
Chemotherapy is a method of oncological treatment involving the administration of a drug or group of drugs designed to neutralize cancer cells, slowing their growth and damaging them. In the case of breast cancer, it can be used either as an adjuvant treatment before surgery, as a complementary treatment after surgery or as a completely separate branch of therapy [5].
Radiotherapy is a treatment method that involves irradiating the tumor site with X-ray radiation. The aim of this method is to damage cancer cells. Adjuvant radiation therapy is the standard treatment recommended for 90% of breast cancer patients. Radiotherapy after breast-conserving surgery is associated with a 22% reduction in 10-year local recurrence and a 5% reduction in 15-year overall mortality [5,6].
Physiotherapy plays a key role in the patient’s recovery period, speeding up the process of returning to fitness. Combination therapy in the form of radiotherapy, chemotherapy and surgery may be associated with complications. These include lymphedema, Axillary Web Syndrome (AWS), upper limb movement restrictions and muscle atrophy. Physiotherapy is one of the primary methods of preventing and treating complications that have already arisen. Treatments using movement as a therapeutic agent (kinesiotherapy), but also physical therapy, therapeutic massage and manual therapy are used [7].
There is little information in the available medical literature about the level of knowledge of physiotherapists as well as physiotherapy students about possible complications related to oncology treatment.
Aim of the work
The aim of the study was a comparative analysis of the level of knowledge of third- to fifth-year physiotherapy students and practicing physiotherapists up to 45 years of age in the field of rehabilitation of post-mastectomy complications.
Material and methods
The study was conducted between 18th May and 1st November 2022. A total of 112 participants (41 physiotherapy students and 71 physiotherapists) took part in the study, with a mean age of 31.10±8.02 years. The largest group of the respondents was from the youngest age group, between 20 and 30 (46.6%). The smallest number of the respondents were in the oldest age group – over 40 (14.9 %).
Sixty-two (54.4%) women and 52 (45.6%) men took part in the survey. In terms of education, the largest group of the respondents were physiotherapists with a master’s degree – 71 (62.4%). Students were the second largest group with 41 (36.6%) people. For students, the largest group of the respondents were fourth-year physiotherapy students with 23 (56.1%) respondents, third-year students with five (12.2%) respondents and fifth-year students with 13 (31.7%) respondents.
The subject evaluation was carried out using a proprietary online survey questionnaire consisting of 31 questions, which was divided into two parts. The first part consisted of 4 questions and asked about socio-demographic characteristics and identifying the source of knowledge on rehabilitation of complications in mastectomy patients. In the question number 6, it was possible to select more than one answer, allowing the respondents to pinpoint different sources of knowledge acquisition. The second part consisted of 25 questions in the form of a test in which only one answer could be marked. One point was awarded for each correct answer and zero points for an incorrect answer. The overall level of knowledge (in terms of points scored) was divided into low (0-13 points), medium (14-19 points) and high (more than 20 points).
The primary test used in the statistical analyses was the Chi-square test of independence of variables, applied to questions built on nominal scales. Coefficients based on the Phi test and Cramér’s V were used to determine the strength of the relationship. The significance of the Phi coefficients and Cramér’s V was determined by the results of the Chi-square test. P≤0.05 was taken as the level of significance.
Results
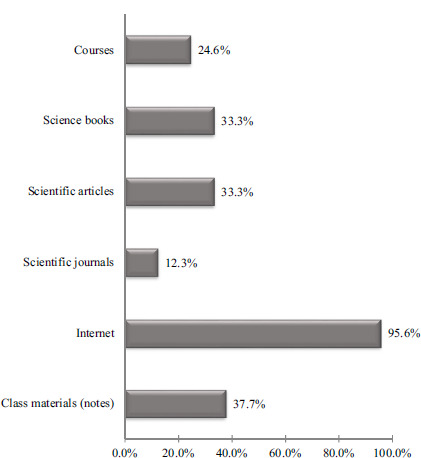
When it came to the sources from which the respondents obtained their knowledge on rehabilitation of post-mastectomy patients, the Internet was dominant, with 109 (95.6%) respondents. Scientific journals were the least frequently selected source of knowledge acquisition among the respondents, indicated by 14 people, representing 12.3% of the respondents. The details are shown in Figure 1.
Based on the number of points scored, moderate levels of knowledge predominated among the respondents – it was recorded in 82 (71.9%) respondents, while the remaining respondents (31 people) were categorized as having low levels of knowledge.
Table 1 shows the respondents’ level of knowledge as assessed by their education, with a maximum score of 25. The student group achieved a low level (0 to 13 points) in 36.6% of cases, while the master’s degree holders did so in 22.5%. In contrast, a moderate level (14 to 19 points) was achieved by 63.4% of students and 77.5% of master’s degree holders. Overall, of all the respondents, 27.7% obtained a low level of knowledge and 72.3% a moderate level. The respondents with a master’s degree were more likely than students to have a higher level of knowledge, but the analysis did not show a statistically significant relationship (p=0.504) between the variables (Table 1).
Table 1
Level of knowledge of the respondents in the context of education
Considering the age of the respondents, a moderate level of knowledge prevailed in all age groups of the respondents. Age did not significantly differentiate (p=0.439) the level of knowledge of the respondents (Table 2).
Table 2
Level of knowledge of the respondents in the context of age
Considering the gender of the respondents, a moderate level of knowledge was obtained by 43 (69.4%) women and 39 (77.0%) men. There were no statistically significant differences (p=0.504) between the study groups (Table 3).
Table 3
Level of knowledge of the respondents in the context of gender
Considering the knowledge of the students in terms of their year of study, a moderate level was obtained by 4 (80%) students from the 3rd year, 12 (52.2%) students from the 4th year and 11 (84.6%) students from the 5th year. Year of study did not statistically significantly differentiate the level of knowledge (p=0.111) (Table 4).
Table 4
Level of knowledge of the respondents in the context of their year of study
No statistically significant relationships were found between the level of knowledge and the respondents’ sources of knowledge on the rehabilitation of complications in patients after breast cancer treatment (Table 5).
Table 5
Level of knowledge of the respondents in terms of sources used
The physiotherapists surveyed were more likely than the students to derive their knowledge of rehabilitation complications in patients after breast cancer treatment from courses (p=0.01), while the students were significantly more likely to derive their knowledge from materials available in classes at the university (p=0.001). Detailed data is presented Table 6.
Table 6
Comparison of sources of knowledge between the groups studied
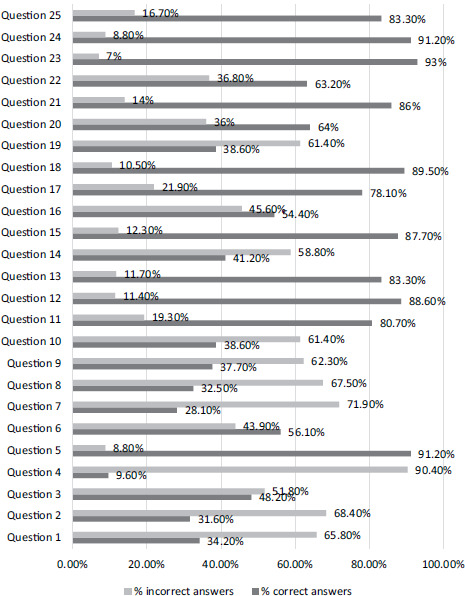
The respondents gave the most correct answers to the question on the effects of large lymphedema after mastectomy, which was correctly answered by 102 respondents, representing 89.5% of the survey participants. The question on the effects of radiotherapy was answered correctly by 95 respondents, or 86%. The question on the use of kinesiotape in lymphatic technique also had a high number of correct answers, given by 89 respondents (78.1%). The next question with the highest number of correct answers was the Stemmer sign question, which was answered correctly by 62 respondents, representing 54.4%.
One question with a low number of correct answers concerned the appropriate positioning of the upper limb after mastectomy surgery. The correct answer was given by 11 (9.6%) respondents. When asked about AWS, 36 (31.6%) respondents answered correctly. When asked about the weakness of the muscles responsible for movement in the upper limb, 32 respondents (28.1%) gave the correct answer. The details are shown in Figure 2.
Figure 2
Summary of correct and incorrect answers to individual questions from the survey
Notes:
Question 1: How much time must pass after the end of oncological treatment for a patient to benefit from sanatorium rehabilitation?
Question 2: What do you think AWS consists of?
Question 3: What should rehabilitation use in the event of AWS?
Question 4: In what position should the upper limb be placed as soon as possible in the event of adduction contracture in the shoulder joint?
Question 5: What will upper limb elevation allow?
Question 6: What is the period of early postoperative rehabilitation in hospital?
Question 7: The muscles responsible for which movements weaken the most after mastectomy and removal of axillary nodes? Question 8: When is verticalization most commonly performed after mastectomy surgery?
Question 9: What is used to prepare the place from which material will be taken for breast reconstruction surgery?
Question 10: Should anticoagulant exercises be used in the postoperative period after mastectomy?
Question 11: Can the pathomechanical chain, beginning with impairment and overloading of the shoulder joint as a result of surgical treatment, cause thoracic and spinal statics and shortening of the muscle?
Question 12: What are the benefits of using breathing exercise equipment?
Question 13: Why are breathing exercises used in the postoperative period?
Question 14: With what frequency should exercises for pulmonary and vascular postoperative complications be performed? Question 15: What are cardiac complications after radio- and chemotherapy?
Question 16: At which test is the Stemmer sign used?
Question 17: What is the stretch of the kinesiotape when using the lymphatic technique?
Question 18: What can cause severe lymphedema?
Question 19: What cannot be used for physical therapy treatments applied in comprehensive decongestion therapy? Question 20: What is not a contraindication to the use of intermittent pneumatic compression?
Question 21: What can treatment with radiotherapy result in?
Question 22: What exercises are not used due to the increased risk of infection?
Question 23: What is recommended to prevent contractures after radiotherapy?
Question 24: What should not be used in the area that has been treated with radiotherapy?
Question 25: There is a reduction in bone mineral density when radiotherapy is used. May this result in osteoporosis, which most often affects bones?
Discussion
There are a number of complications with oncological treatment of mastectomy patients, which include AWS, lymphedema, adduction contracture and muscle atrophy. Through the process of rehabilitation, their incidence is reduced and physiotherapy treatments are one of the main methods of treating complications after breast cancer treatment [7].
In the present study, the respondents scored an average of 14.89 points in a test of 25 questions, indicating a moderate level of knowledge. Those with a master’s degree were more likely than students to have a higher level of knowledge, but the analysis did not show a statistically significant relationship between these variables. Despite the lack of correlation between the level of knowledge and the sources of knowledge, it is worrying that the respondents were least likely to use scientific journals.
Upper limb lymphedema, which is associated with surgery and radiotherapy for breast cancer, occurs in 24% to 49% of cases and may be present immediately after surgery or build up years after surgery. Most edema-related complications occur during the first 18 months after surgery and radiotherapy [7]. Reduced lymphatic transport, which often occurs in the upper limb when surgery is performed, increases the risk of infection, fibrosis, impingement syndrome, skin lesions, decreased sensitivity and function in affected individuals [8]. The presence of lymphedema can cause pain, weight gain of the affected limb and deformities and secondary problems such as cellulitis and thrombosis [7]. Lymphatic accumulation is able to exert pressure on the brachial plexus and consequently cause complications in the form of sensory disturbances, paresthesia and muscle paralysis. The correct answer to this question on the effects of edema was marked by 89.3% of the respondents. The high percentage of correct answers may be due to the fact that lymphedema is the most common complication, which is widely discussed in the study program and scientific literature [9,10].
The question on negative effects resulting from radiotherapy was also one of the questions best answered by the respondents (86% gave the correct answer – fibrosis of the skin and subcutaneous tissue, swelling of the upper limb and brachial plexus damage). The toxicity of chemotherapy or radiotherapy significantly affects both the quality of life and premature death of patients. Experts at The National Cancer Institute in the USA have identified cardiotoxicity of anticancer treatment as a significant complication affecting the heart. It is observed in a patient population with a long-term survival of 5-10 years, particularly in women with breast cancer [11]. The most common cardiovascular dysfunctions that can occur during anticancer treatment are left ventricular dysfunction, heart failure, myocardial infarction, cardiac rhythm or conduction abnormalities, acute myocarditis or pericarditis, hypertension or hypotonia and, in the case of radiotherapy, coronary artery disease [12].
The application of kinesiotaping patches makes the skin slightly elevated, which simultaneously increases the space between the dermis and fascia causing a reduction in lymphatic stasis and swelling [13]. If a lymphatic application is used, the suggested stretch of the patch is between 15 and 25% [14]. The question regarding the stretching of the tape with the lymphatic method was answered correctly by 78.1% of the respondents. This may be due to the widespread use of kinesiotaping, the easy methodology of the treatment and the fact that it is introduced as early as the college education stage.
Another question that was answered correctly by 54.4% of the respondents concerned the Stemmer sign. The Stemmer sign test involves grasping a fold of skin near the proximal phalanx of the second or third finger and lifting it upwards. If it cannot be lifted or even grasped, this sign is considered positive, suggesting lymphedema, which on average affects 20-30% of breast cancer patients after removal of axillary lymph nodes and adjuvant radiotherapy [15]. The number of correct answers to this question may be due to the fact that a given symptom is quite common, and therefore the respondents may have already encountered it during student internships or in clinical practice.
The correct positioning of the upper limb is an essential part of the rehabilitation process for post-mastectomy patients. It is introduced already in the hospital period and is one of the necessary recommendations to be followed after the patient leaves hospital [16]. By correctly positioning the upper limb on the side of the amputated mammary gland and the adjacent upper axillary nodes, lymphatic stasis, which is one of the biggest problems for patients after mastectomy, is prevented. It is advisable to position the upper limb in abduction and to use a wedge under it. The results of the study show that the question regarding the correct positioning of the upper limb used when adduction contracture occurs was the most difficult for the respondents, with 87.9% of the students and 91.5% of the physiotherapists answering it incorrectly. A study by Kaźmierczak et al. [17] confirms that breast amputation is a cause of mobility limitations in the shoulder joint. The most common limitation of mobility was in the movement of abduction [17].
One of the questions to which the respondents gave the most incorrect answers related to the AWS. The number of correct answers among the 112 people was 35 (30.4%). AWS or cording is a dysfunction that usually occurs between the first and fifth week after surgery. It is characterized by the presence of a visible and palpable stretched band under the skin, which is tight and painful during shoulder flexion or abduction movements [18,19]. The cords are always present in the axillary fossa and may extend to the medial ipsilateral shoulder. AWS is observed with the presence of two or three palpable cords under the skin, without congestion, with increased local temperature or systemic symptoms such as significant loss of range of motion in the upper limb, numbness, pain and pressure mainly when performing arm abduction [20]. The number of incorrect answers may have been due to the infrequent coverage of AWS during physiotherapist education.
The next question that caused most problems for the respondents related to the weakness of the muscles responsible for upper limb movements. The correct answer to this question was given by 28.1% of those surveyed. The most restricted movements are straightening, abduction, external rotation and internal rotation of the arm [21]. One of the problems patients face after breast tumor removal surgery is pain. In order to prevent pain, patients often adopt a pain-relieving position through adduction and flexion at the shoulder and glenohumeral joint. As a result of prolonged maintenance of this position, muscle atrophy occurs, mainly responsible for the movements of horizontal straightening, abduction, as well as external and internal rotation of the arm [16].
An integral part of conducting rehabilitation, especially for patients after surgery, is kinesiotherapy. In the early stages after chemo- and radiotherapy treatment, exercise in water is not recommended. When using the above oncological treatment methods, the immune system weakens [22-24]. In our study, 26 (23.2%) respondents indicated water exercise as contraindicated due to the increased risk of infection in women after breast cancer treatment.
Medical literature describes that physical therapy is recommended on average 5 years after completion of oncological treatment [16,24,25]. According to the definition, spa treatment is an organized activity consisting of the provision of health care services, carried out in a spa using natural conditions, such as the properties of natural medicinal raw materials, curative properties of the climate. Nevertheless, the question regarding the provision of sanatorium rehabilitation in post-mastectomy patients proved problematic. The correct answer, 1 year, was marked by 33.9% of the respondents. The number of incorrect answers may suggest that the respondents marked a later period of rehabilitation based on their previous knowledge and recommendations for physical therapy.
The results of the study indicate that the level of knowledge of physiotherapy students and physiotherapists about rehabilitation and complications after mastectomy is moderate. It is important that students and physiotherapists, who want to treat their patients effectively, should successively deepen their competences by attending conferences and training courses and regularly read current scientific publications in this field.
Conclusions
Analysis of the results obtained led to the following conclusions:
The Internet was the main source of knowledge about the rehabilitation of mastectomy patients. The importance of verifying the quality of online information should be emphasized.
Scientific journals were the least popular source of information, which may indicate the need to promote their value in terms of providing reliable information.
A moderate level of knowledge was predominant, indicating an overall average state of knowledge among the groups surveyed.
There were no statistically significant differences in the level of knowledge in relation to age, gender or the sources of knowledge used, which may suggest that factors other than those studied have a greater influence on knowledge about rehabilitation after mastectomy.
There is a need for more diverse educational methods to improve knowledge in areas identified as weaknesses.