









Introduction
The balance between energy and protein intake and energy expenditure, which ultimately determines a patient’s nutritional status, is regulated by many factors, one of which is the balance between orexigenic (e.g., orexin and neuropeptide Y) and anorexigenic (e.g., leptin) peptides (mainly) in the central nervous system [1–3]. Recent data show that orexin, in addition to regulating appetite (food intake) and energy homeostasis, may take part in a variety of physiological functions, through its activity in both the central and peripheral nervous systems [4, 5]. Through its activity in the central nervous system, orexin regulates sleep and wakefulness [4–6], stress reactions [7], addiction to cocaine, opioids, amphetamines, cannabis, alcohol and nicotine [4, 5, 8–10], reward seeking, motivation and memory; and, through its activity in the peripheral nervous system, regulates blood pressure, hormone secretions, reproduction, gut motility and lipolysis [4, 5, 11]. By the pathomechanisms mentioned, low orexin-A/hypocretin-1 and orexin-B/hypocretin-2 levels and the low expression of their receptors, OX1R and OX2R, participate in the pathogenesis of type I narcolepsy, neuro- and chronic inflammation, neurodegenerative diseases and metabolic syndrome, as well as in the stimulation of pain, inflammation, and carcinogenesis [4, 5] and cancer-related angiogenesis, inter alia, through the stimulation of vascular endothelial growth factor A (VEGF-A) [12–15]. Orexin-1 receptors were found in both digestive (colorectal cancer [CRC], pancreatic ductal adenocarcinoma, hepatocellular carcinoma [HCC], gastric cancer, esophageal cancer and cholangiocarcinoma) and non-digestive (prostate cancer, neuroblastoma, cortical adenomas, pheochromocytomas and endometrial carcinoma) cancers [5]. Low orexin blood concentration has been associated with cancer resistance to chemotherapy (especially to 5-fluorouracil and gemcitabine) [4, 5, 12] and to anti-angiogenic therapy (e.g., bevacizumab in patients with CRC) [13–15], as well as being associated with a risk of acute kidney injury induced by cisplatin in mice [16]. It was reported that orexin-knockout mice (i.e., with orexin deficiency) were susceptible to diet-induced obesity, liver steatosis, and progression to non-alcoholic steatohepatitis (NASH) and HCC [17]. In other studies, high orexin-A blood concentration or daily orexin administration: suppressed the expression of exosomal PD-L1 in CRC and promoted T-cell activity by inhibiting the JAK2/STAT3 signaling pathway (anti-cancerogenic activity) [18]; exerted an analgesic effect in a murine model of chemotherapy-induced peripheral neuropathy (CIPN) [7]; prevented NASH and HCC in orexin-knockout mice and obese human patients [4, 5, 14, 17]; regulated glucose metabolism in HCC cells [19]; regulated cancer cell apoptosis [20]; induced autophagy in HCT-116 human colon cancer cells through the extracellular signal-regulated kinases (ERK) signaling pathways [20]; and promoted tumor apoptosis in vivo [4, 5, 21, 22]. Therefore, the orexin receptor OX(1)R has been recognized as a promising therapeutic target for CRC patients [23], as well as for multiple pathologies related to inflammation, including intestinal bowel disease, multiple sclerosis, septic shock and obesity [4, 5]. To date, only orexin receptor antagonists approved for insomnia treatment are available on the market (suvorexant, lemborexant, daridorexant and almorexant) [4–6].
Aim
Taking into account the orexin properties enumerated above, our study, which to the best of our knowledge is the first in humans, determined the blood orexin concentration in consecutive patients undergoing surgery for CRC, focusing on its relation to the patients’ nutritional status, clinical cancer stage, treatment complications and prognosis.
Material and methods
Patients
The study involved 84 consecutive inpatients with primary CRC who underwent elective surgery between 2016 and 2019 at our University Hospital. The exclusion criteria were lack of informed consent to participate in the study and the need for emergency surgery (e.g., due to bowel obstruction or hemorrhage).
During their first day of admission, a medical history was obtained from each of the patients enrolled in the study, and a physical examination was performed that included an assessment of anthropometric parameters of nutritional status and body composition (described in the subsection below). Data concerning tumor size, clinical and histopathological stages, and perioperative complications were also collected. After being discharged, the patients were invited to attend a follow-up visit 3 months after their operation. All the examinations performed during the baseline visit were repeated during the follow-up visit. In the long-term follow-up (median: 1322.0; IQR: 930.6–1788.5 days; mean: 3.6 years), the patients’ survival status was checked during a telephone visit.
Parameters of nutritional status and body composition assessment
The following parameters of nutritional and anthropometric status assessment were measured at baseline and at the 3-month follow-up visit: Nutritional Risk Screening (NRS)-2002 (a score of 3 or more points in the questionnaire indicating a risk of malnutrition-related complications); Patient-Generated Subjective Global Assessment (PG-SGA) (a score of 5 or more points in the questionnaire indicating a risk of malnutrition-related complications); Mini Nutritional Assessment (MNA) (a score in the range 17–23.5 in the questionnaire indicating a risk of malnutrition, and a score < 17 indicating malnutrition); body weight (kg); height (cm); body mass index (BMI) (kg/m2) (measured as the ratio of body weight to the square of height (m)); waist circumference (WC) (cm); waist-to-height ratio (WHtR) (measured as the ratio of WC (cm) to height (cm)); mid-arm circumference (MAC) (cm); calf circumference (cm); triceps skinfold thickness (TSF) (mm) and subscapular skinfold thickness (SST) (mm) (measured using the Harpenden MG-4800 manual skinfold caliper; BATY, UK); and the handgrip strength (HGS) (kg) of the dominant hand (measured using an electronic dynamometer; Kern, Germany). Normal cutoff values for HGS were established as 20 kg for females and 30 kg for males. Body composition was determined using whole-body bioelectrical impedance analysis (BIA) with a TANITA BC 420 MA device (TANITA Corporation, Japan). The following BIA parameters were analyzed: fat mass (FM) (expressed as a percentage of total body weight [FM%] and as absolute mass in kg [FM, kg]); visceral adipose tissue (VAT) score (range: 1–59, a level > 12 showing abdominal adiposity); fat-free mass (FFM) (kg); skeletal muscle mass (SMM) (expressed as a percentage of total body mass [SMM%] and as absolute mass in kg [SMM, kg]); basal metabolic rate (BMR) (kcal); and metabolic age (MA) (years). Moreover, because abdominal computed tomography (CT) was performed in every CRC patient before surgery (range of slice thickness: 1–5 mm), the regional densitometric quantification of skeletal muscle (SM) (attenuation limit –30 to 150 Hounsfield units [HU]), VAT (attenuation limit –150 to –50 HU) and subcutaneous adipose tissue (SAT), and their cross-sectional areas at the third lumbar (L3) vertebra were manually selected using OsiriX software (Pixmeo SARL, Bernex, Switzerland) as specific regions of interest (ROI) [24] and parameters of body composition.
Functional status, using, for example, the Barthel index, activities of daily living (ADL) and Instrumental Activities of Daily Living (IADL) indices, was also completed.
Biochemical determinations
Blood samples were taken from the ulnar vein of each patient between 7 am and 8 am on the day of admission while they were in a fasting state. For all patients in the study, the following biochemical determinations were performed in the hospital’s diagnostic laboratory using standard methods: blood morphology with a detailed determination of white blood cell distribution (total lymphocyte count [TLC] and neutrophils), glucose, albumin, C-reactive protein (CRP), and carcinoembryonic antigen (CEA). The Preoperative Onodera’s Prognostic Nutritional Index (OPNI) was also calculated according to the following formula: [10 × blood albumin concentration (g/l)] + [0.005 × TLC (G/l)] [25].
Serum orexin concentration was assessed using an immunoenzymatic ELISA kit from Cloud-Clone Corp. (cat. no. CEA607Hu), in accordance with the manufacturer’s instructions. Serum samples were centrifuged at a temperature of 4°C with a spin speed of 3500 revolutions per minute. The serum sample was then stored at a temperature of –80°C until determination.
Measured outcomes
At the beginning of the study, the following were measured: blood orexin concentration, initial (preoperative) values of nutritional status assessment and body composition parameters (BIA, CT), scores in patient’s functional status questionnaires, length of in-hospital stay (LOS), occurrence of perioperative complications, cancer localization (rectum, colon) and stage (WHO clinical stages, I-IV). At the 3-month follow-up visit, as at baseline, nutritional and functional status questionnaires were completed, and anthropometric parameters of nutritional status and BIA parameters of body composition obtained. In the long-term follow-up, patients’ survival was checked by a telephone visit in May, 2022, with a median follow-up period of 1322.0 (IQR: 930.6–1788.5) days (mean: 3.6 years).
Statistical analysis
Statistical analysis was conducted using the licensed version of the statistical software Statistica, version 13.3, developed by Tibco Software, Inc. (2017). The normal distribution of the study variables was checked using the Kolmogorov-Smirnov test. Depending on the type of variable distribution, the results were presented as: the median; the interquartile range (IQR); the mean ± standard deviation; or n, %; and the statistical significance of differences between groups was verified using the Mann-Whitney U non-parametric test, Student’s t-test, or χ2 test. The statistical significance level was set at a p-value < 0.05. A Kaplan-Meier curve was determined in the survival analysis. We also used a ROC curve with the lowest Youden’s index and the area under the curve (AUC) with 95% confidence interval (CI) to determine the cutoff values of the blood orexin concentration in prediction of outcomes measured. Spearman correlation between studied parameters was determined.
Results
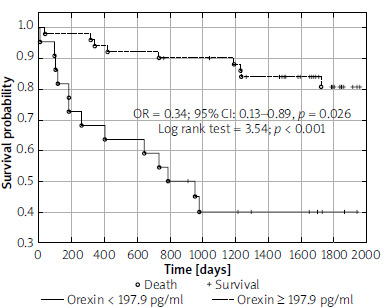
During 1296 ±617.7 days of follow-up (on average 3.7 years) of 84 CRC patients studied, 27 (32.1%) died. In ROC curve analysis we found the blood orexin concentration cutoff of 197.9 pg/ml, which was predictive for all-cause mortality during long-term follow-up (AUC = 0.626; 95% CI: 0.498–0.755; p = 0.049), and increased nutritional risk (defined as NRS2002 ≥ 3) at the 3-month visit after colorectal cancer surgery (AUC = 0.746; 95% CI: 0.611–0.882; p < 0.001). Based on this cutoff, we compared parameters obtained between CRC patient groups with lower and equal to or higher blood orexin concentration.
Orexin and baseline parameters of patients’ nutritional status assessment
Compared to CRC patients with a serum orexin concentration lower than the established cutoff (197.9 pg/ml), those with orexin concentrations equal to or higher than the cutoff value predictive for long-term all-cause mortality were, at baseline, more likely to have a higher baseline blood orexin concentration, higher score on MNA, Geriatric Nutritional Risk Index (GNRI), Nutritional Risk Index (NRI), OPNI, Barthel, IADL scales, greater HGS, and were more likely to have HGS above the established cutoff suggesting sarcopenia, higher blood albumin concentration, to have a higher mid-arm circumference, mid-arm muscle area, and higher fat-free mass in BIA (Table I). Moreover, compared to CRC patients with a serum orexin concentration lower than the established cutoff value, those with a serum orexin concentration equal to or higher than 197.9 pg/ml had significantly lower NRS2002 and PG-SGA scores, percentage of preoperative weight loss, CRP, and CRP to albumin ratio (Table I). When we performed the same comparisons, i.e. between subgroups with blood orexin concentration lower and equal to or higher than 197.9 pg/ml (the cutoff value obtained in ROC analysis), separately for patients with rectal and colon cancer, we obtained similar results, i.e. in both patient subgroups those with higher blood orexin concentration had more favorable values of parameters of nutritional and functional status assessment (data not presented in detail).
Table I
Baseline clinical characteristics of patients with blood orexin concentration higher than or equal to, and lower than, the cutoff value obtained in ROC analysis (197.9 pg/ml), predictive for long-term mortality
[i] ADL – activities of daily living, CRP – C-reactive protein, CT – computed tomography, GNRI – Geriatric Nutritional Risk Index, IADL – Instrumental Activities of Daily Living, HGS – handgrip strength, L3 – third lumbar vertebra, MNA – Mini-Nutritional Assessment, NRI – Nutritional Risk Index, NRS-2002 – Nutritional Risk Screening questionnaire 2002, OPNI – Onodera’s Prognostic Nutritional Index, PG-SGA – Patient-Generated Subjective Global Assessment. Data presented as: mean ± standard deviation, median (IQR), or n, %.
Moreover, in ROC analysis performed for the whole study group, we determined the predictive value of baseline blood orexin concentration for: normal SM percentage in BIA analysis at baseline with an orexin cutoff of 464.7 pg/ml (AUC = 0.350; 95% CI: 0.218–0.480; p = 0.025), history of body weight loss > 5% of usual body mass at baseline with an orexin cutoff of 464.70 pg/ml (AUC = 0.134; 95% CI: 0.022–0.246), achievement of HGS above gender-specific cutoffs suggesting sarcopenia at baseline with a blood orexin concentration cutoff of 579.4 pg/ml (AUC = 0.219; 95% CI: 0.110–0.329; p < 0.001), and postoperative complications occurrence with a blood orexin concentration cutoff of 217.4 pg/ml (AUC = 0.754; 95% CI: 0.636–0.873; p < 0.001).
In the whole study group, initial blood orexin concentration corelated statistically significant with the following parameters obtained at the study beginning: HGS (R = 0.44; p < 0.001), IADL score (R = 0.40; p < 0.01), blood albumin concentration (R = 0.25; p = 0.023), SM mass in BIA (R = 0.33; p = 0.002); SM cross sectional area (CSA) at L3 by CT (R = 0.27; p = 0.016). The correlation between blood orexin concentration and SM CSA was statistically significant in patients with rectal cancer (R = 0.40; p = 0.023), but among patients with colon cancer such a relationship was not confirmed.
Orexin and parameters of CRC stage and surgery outcomes
No statistically significant differences in tumor size, clinical stage, metastases to lymph glands, stage according to the Astler-Coller classification, WHO stage, or histopathological malignance grade were found between CRC patient groups divided according to orexin blood concentration (Table II). Such associations were also not found in ROC and regression analyses.
Table II
Prevalence of outcomes measured and parameters of colorectal tumor size and clinical stage in patients with blood orexin concentration higher than or equal to, and lower than, the cutoff value obtained in ROC analysis (197.9 pg/ml), predictive for long-term mortality
Compared to CRC patients with a serum orexin concentration lower than the established cutoff value predictive for all-cause mortality during 3.6-year follow-up, those with a serum orexin concentration equal to or higher than the assumed cutoff had a lower proportion of all-cause mortality and whole perioperative complications (Table II). Patients with a higher blood orexin concentration required a lower number of units of blood transfused in the perioperative period.
Orexin and parameters of patients’ nutritional status assessment at a 3-month visit
At the 3-month follow-up visit, compared to CRC patients with a serum orexin concentration lower than the cutoff value predictive for all-cause mortality during follow-up, those with a serum orexin concentration equal to or higher than 197.9 pg/ml had significantly higher Barthel and IADL scores, HGS, mid-arm and calf circumference, visceral adiposity score and SMM in BIA, a significantly lower NRS2002 score and a lower percentage of patients with malnutrition risk, defined as NRS2002 ≥ 3 (Table III). The associations between blood orexin concentration at the beginning of the study and nutritional risk (defined as NRS2002 score ≥ 3) and lack of achievement of normal HGS at the 3-month visit were also confirmed in ROC analysis with cutoffs of 197.9 pg/ml (AUC = 0.746; 95% CI: 0.611–0.882; p < 0.001) and 202.90 pg/ml (AUC = 0.682; 95% CI: 0.547–0.817), respectively. Blood orexin concentration at the start of the study corelated with mid-arm circumference (R = 0.31; p = 0.011) and SM mass in BIA (R = 0.43; p < 0.001) at the 3-month visit. In patients with rectal cancer the relationship between baseline blood orexin concentration and SM mass in BIA at the 3-month visit was stronger (R = 0.63; p < 0.001), but in patients with colon cancer it was not statistically significant.
Table III
Parameters of nutritional status assessment 3 months after surgery for colorectal cancer in patients with blood orexin concentration higher than or equal to, and lower than, the cutoff value obtained in ROC analysis (197.9 pg/ml) predictive for long-term mortality
Orexin and outcomes measured after long-term follow-up through a telephone visit
After, on average, 1296 ±617.7 days of follow-up, 27 (34%) of the patients had died. Compared to CRC patients with a serum orexin concentration lower than 197.9 pg/ml, those with a serum orexin concentration equal to or higher than the established cutoff were significantly less likely to suffer all-cause mortality during the follow-up period (Table II).
In logistic regression analysis, we also found that baseline serum orexin concentration was associated with a reduced risk of all-cause mortality (OR = 0.34; 95% CI: 0.13–0.89; p = 0.026). This observation was also confirmed in survival analysis using a binary Kaplan-Meier curve (log rank test 3.54; p < 0.001) (Figure 1).
Discussion
To the best of our knowledge, our study is the first worldwide to assess the role of orexin concentration in humans. We found that CRC patients undergoing surgery had different serum orexin concentrations, and that the level of this orexigenic peptide, a biomarker of energy homeostasis, was associated with patients’ nutritional status, both at baseline (Table I) and at a 3-month follow-up visit (Table III). Moreover, blood orexin concentration was associated with a risk of perioperative complications and all-cause death during, on average, 1296.0 ±617.7 days of follow-up (Tables I, II, Figure 1).
Orexin, as a peptide determining, among other factors, a patient’s appetite and food intake, as well as the development and progression of inflammatory and cancerous diseases, was investigated in humans only recently, and earlier work was done on animals [4, 5] or in vitro models [18]. Therefore, there are no studies available with which we could compare the results we obtained, both with regard to patients’ prognosis and to changes in patients’ nutritional status and risk (Tables I, III). Nevertheless, our study suggests that higher baseline blood orexin concentration is associated with a higher percentage of patients surviving 3.6 years after surgery for CRC (Table II, Figure 1), lower risk of all-cause and non-surgical perioperative complications (Table II), as well as better nutritional and functional status, expressed by higher skeletal muscle mass, strength, and performance, both before surgery and at the 3-month visit (Tables I, III). The positive relationships between blood orexin concentration and reduced risk of sarcopenia, frailty and/or cachexia [25] were also confirmed by Spearman correlations of blood orexin concentration with SM mass in BIA, SM CSA in CT, and scores in functional scales. Because the majority of studied patients were male, the use of BIA for body composition analysis seems to be reliable, especially as all examinations were performed at a similar time with similar conditions of patient hydration, the observed associations between orexin and body composition parameters concerned fat-free and SM mass, and the mentioned associations were also found in CSA analysis of SM by CT. A potential pathophysiological explanation for these associations may be the following characteristics of orexin: anti-inflammatory and anti-cancerogenic properties [18], improving or maintaining normal physical activity, nutritional status, appetite, food oral intake and energy homeostasis (cancer cachexia prevention) [4, 5, 21, 25], sleep regulation [6, 26–28], lower risk of narcotic bowel syndrome, and opioid withdrawal symptoms [4, 5, 8–11].
As stated above, in none of the available papers did we find data concerning the prognostic value of blood orexin concentration in CRC patients (reduced all-cause mortality risk by on average 66%), although hypocretin (orexin) neuropeptide precursor (HCRT) gene methylation was revealed as a biomarker of recurrence and prognosis in patients with head and neck neoplasms [29], and, in patients with mild-to-moderate acute ischemic stroke, blood orexin concentration was positively associated with patients’ prognoses [30]. In our study, the factors with the potential to explain the better prognosis and lower risk of perioperative complications among CRC patients with a higher blood orexin concentration might be their better quality of sleep [6, 26–28], maintenance of normal nutritional and functional status (Tables I and III) and of appetite and oral food intake [25], as well as a smaller inflammatory response (Table I). A previous study revealed that, as with orexin, clinical value may also be found in blood adipocytokine concentration (e.g., adipokine and TNF-α), which is related to cancer clinical state, probability of radical tumor excision, occurrence of non-surgical postoperative complications, and long-term survival [31].
In our study, we only found some associations between patients’ perioperative course and serum orexin concentration (Table II); however, none of the relationships concerned serum orexin concentration and CRC stage (Table II). In a study by Tsuneki et al. [17] on orexin-knockout mice, orexin deficiency was related to the progression of pre-cancerous conditions to neoplasm. Anti-cancerogenic properties of orexin investigated in animal studies were also reviewed by Couvineau et al. [4, 5], and supported by other authors cited in the introduction section, including works on orexin supplementation [12–15, 17–22, 32–36]. Orexin or orexin receptor agonist application might also potentially help to improve or maintain patient nutritional and functional status and prevent sarcopenia, cachexia and frailty.
As with the majority of studies, our analysis has some shortcomings that may reduce the strength of the conclusions obtained. The small number of patients included in our study should be considered the main limitation. The small sample size made it impossible to perform a separate analysis for patients with rectal and colon cancer. Nonetheless, the novelty of this study is unquestionably a strong point: to the best of our knowledge, in the first study worldwide to assess the role of orexin concentration in humans, we observed a favorable effect of higher serum orexin concentration on nutritional status parameters and prognosis in patients undergoing surgery for CRC in one center.
Conclusions
Serum orexin concentrations were found to have statistically significant associations with patients’ nutritional risk and status, concerning mainly skeletal muscle mass and strength, both before surgery and at a 3-month follow-up visit, as well as with all-cause mortality during the 3.6-year follow-up.