







Introduction
According to the GLOBOCAN database, there were approximately 1.774 million emerging colorectal cancer cases around the world in 2018, which makes it the second most widespread cancer in the world [1]. Rectal tumor is a common malignant tumor of the digestive tract, and its incidence rate and mortality rate are in the forefront of digestive system tumors. The treatment methods for early rectal cancer mainly include endoscopic therapy and surgical surgery. The classic endoscopic treatment method is endoscopic submucosal dissection (ESD), which has the advantages of a large resection range and low recurrence rate. However, there are many intraoperative complications and technical difficulties [2]. In recent years, transanal endoscopic microsurgery (TEM) has been widely used as an emerging endoscopic treatment method in the early treatment of rectal tumors [3]. TEM technology achieves the removal and repair of the rectal mucosa and muscle layer in vitro by inserting a working sleeve into the rectum, which has the advantages of minimal trauma, fewer complications, and high tumor clearance. Related studies have shown that the efficacy of TEM in treating early rectal tumors is comparable to traditional open surgery, but with less trauma [4]. However, previous studies on TEM and ESD have been low sample size studies, and the accuracy of their conclusions is insufficient. For this reason, we carried out a meta-analysis to collect relevant case-control study and compare the R0 resection rate, recurrence rate and postoperative complication rate of TEM and ESD for colorectal tumors. This is to assess the clinical curative effect and security of the two methods, and give a new evidence-based medicine basis for treating the colorectal tumors early.
Material and methods
Literature inclusion criteria
(1) The research subjects were patients with rectal tumors. (2) Research intervention measures include TEM or ESD treatment. (3) The design of the study was randomized controlled trial (RCT) or case-control study (CCS). (4) At least one of the following was reported: R0 resection rate, postoperative perforation, bleeding incidence, or tumor recurrence rates as the research results. (5) The research language is English or Chinese.
Exclusion criteria for literature
(1) The study subjects are patients with other tumors or metastatic tumors. (2) The research intervention measures include TEM or ESD combined with other treatment methods. (3) Repeated published research.
Document retrieval strategy
To comprehensively collect the CCS of TEM and ESD treatment of colorectal tumors, this study searched Medline, Embase, Cochrane Library, PubMed and CNKI databases. In the Medline and Embase databases, the search used the following topic word combinations: (“transanal endoscopic microsurgery” [MeSH], TEM [tiab], “endoscopic submucosal dissection” [MeSH] or ESD [tiab]) and (“colonic neoplasms” [MeSH], “rectal neoplasms” [MeSH], “colorectal neoplasms” [MeSH], “colorectal tumor” [tiab] or “colorectal carcinoma” [tiab]). In Cochrane Library and PubMed, the search used the following subject headings: TEM, “endoscopic submucosal dissection” and “colorectal neoplasms”. CNKI was searched using the Chinese theme words corresponding to “TEM, ESD, and Real tumor”. At the same time, we manually searched for references to relevant literature in order to obtain more potential research. The search deadline is for each database to be built until June 2019. The language is limited to English and Chinese. RCT and CCS were selected as the study types. Two reviewers independently screened and evaluated the retrieved literature. Any differences were resolved through negotiation. The two researchers independently searched for literature, read titles and abstracts, and excluded duplicate studies and literature that did not satisfy the standards. They evaluated the full text of the remaining literature, referred to the inclusion criteria, and any differences between the two researchers were resolved through discussion. Design of data extraction table: The two researchers independently extracted the research characteristics (research design, sample size, age, sex ratio, tumor type and stage, etc.) and key indicators (R0 resection rate, postoperative complication rate, tumor recurrence rate and hospital stay). Disagreements were resolved by reviewing the original text.
Literature quality evaluation
The study used Cochrane risk assessment tool to judge the quality of RCT, mainly involving randomized methods, matching hiding, baseline data differences between groups, blind design, incomplete data processing and selective reporting. The quality of CCS was assessed by the CASP tool, including study design, variable validation and control, result analysis and conclusion. The research was rated as high, medium, or low quality.
Statistical analysis
This study used Stata 12.0 software for statistical analysis. We compared the differences in R0 resection rate, postoperative complication rate, and tumor recurrence rate between the TEM group and the ESD group using standardized mean difference (SMD) and its 95% confidence interval (CI) as efficacy measures. P < 0.05 indicates a significant difference. Testing the statistical heterogeneity (SH) between studies, I2 = 0 indicates no statistical heterogeneity; I2 = 50% means moderate heterogeneity; I2 > 50% means obvious heterogeneity. If there was no SH between studies, a fixed effects model (FEM) was used; otherwise, a random effects model was used. A funnel plot was used to test the possibility of publication bias. Sensitivity analysis was conducted to evaluate the robustness of research results. According to the sample size and other factors, the study was divided into different subgroups for subgroup analysis. We compared whether there were differences in the magnitude of effects between different subgroups.
Results
Characteristics of included literature and demographic data of patients
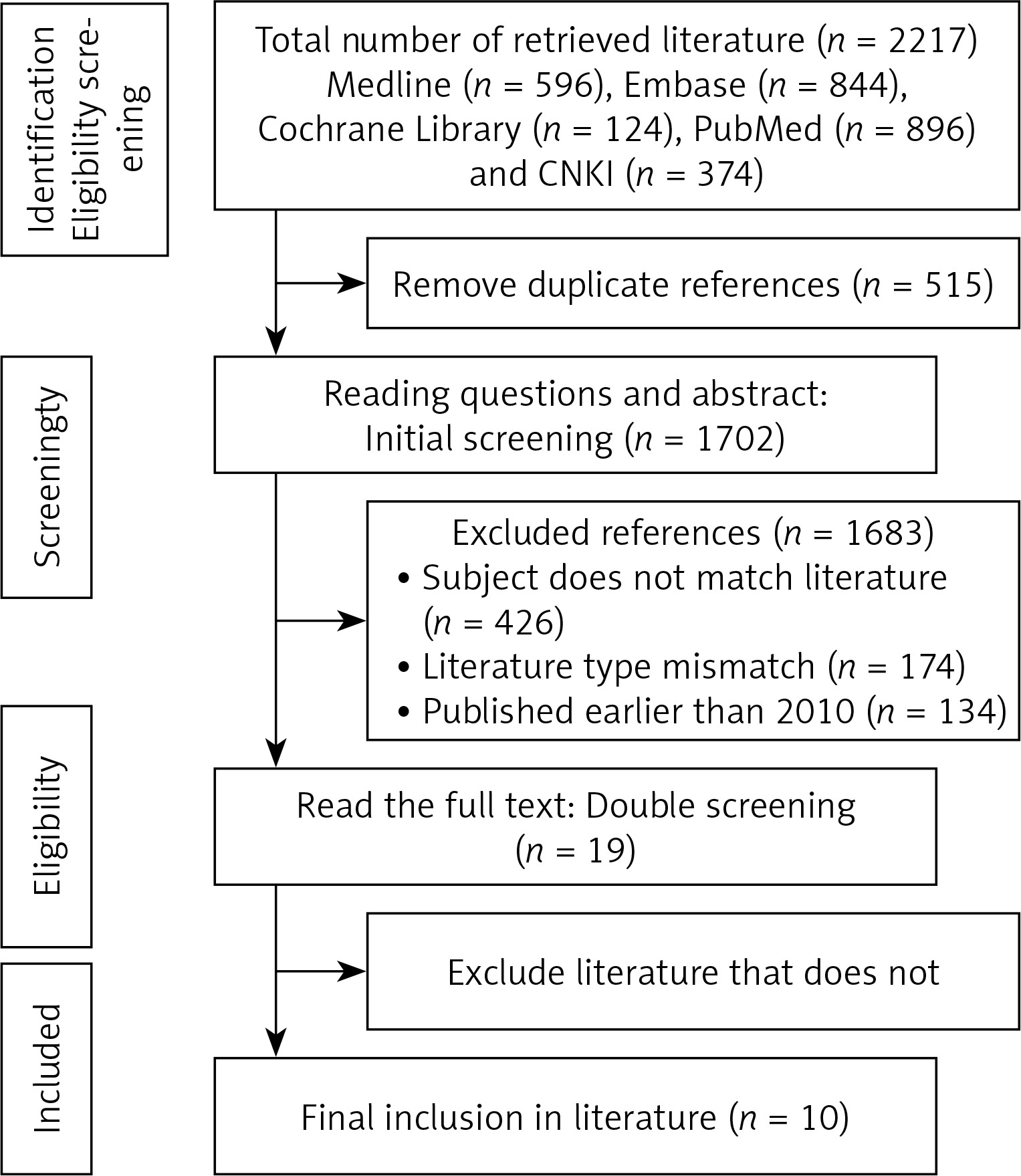
Characteristics of included literature and demographic data of patients were presented in Tables I, II and Figure 1 [5–14].
Table I
Specific features of inclusive literature
| Study | Year | Country | Type of research | Research level |
|---|---|---|---|---|
| Park [5] | 2012 | Germany | Retrospective analysis | Medium |
| Kawaguti [6] | 2014 | Germany | CCS | Medium |
| Mao [7] | 2017 | United States | Non-randomized studies | Medium |
| Jung [8] | 2018 | India | Retrospective analysis | Medium |
| Barendse [9] | 2018 | England | Non-randomized studies | Medium |
| Hon [10] | 2011 | Germany | Matched cohort study | High |
| Yan [11] | 2016 | China | Matched cohort study | High |
| Kiriyama [12] | 2011 | Australia | Retrospective analysis | Medium |
| Jeon [13] | 2014 | Australia | Retrospective analysis | Medium |
| Park [14] | 2021 | United States | Retrospective analysis | High |
Table II
Basic information of included literature
Inclusion of literature quality evaluation results
All studies were retrospectively analyzed. Only 3 out of 10 papers described the propensity score matching method or matching queue, and the data collection was complete; the source of data bias is unclear.
Meta-analysis outcomes
Recurrence
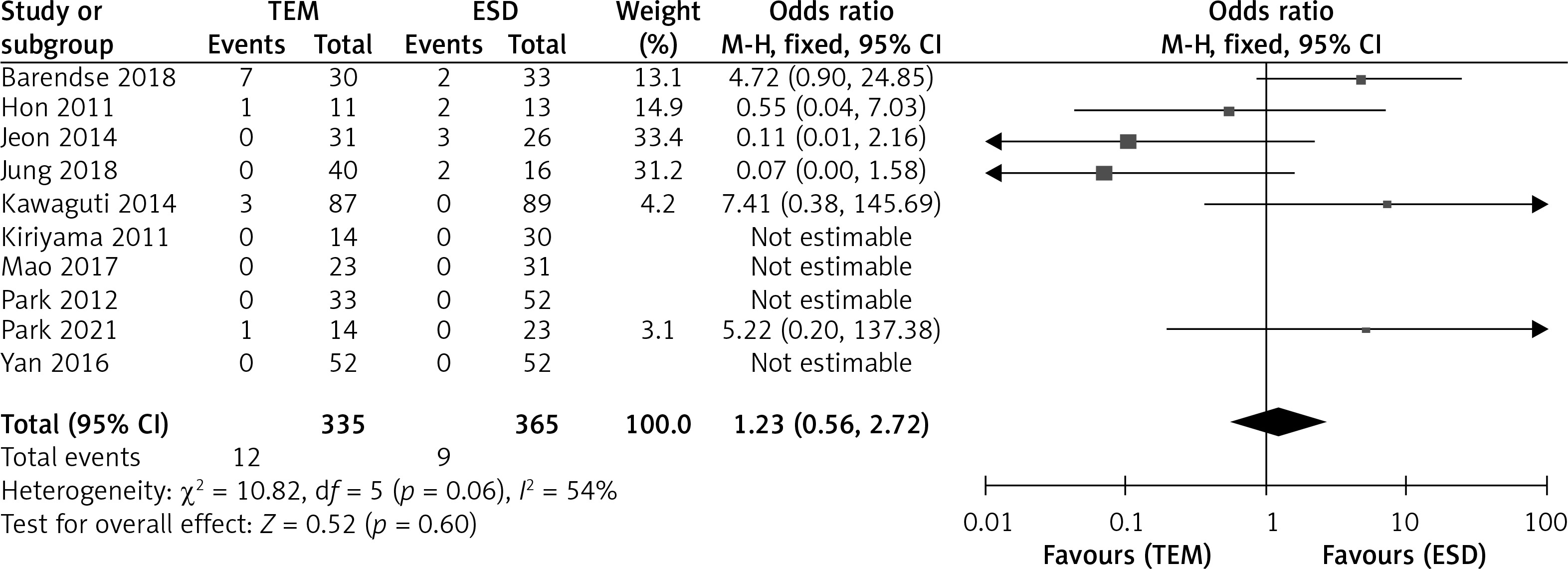
Among the 10 literature reports, 4 were non-recurrent patients, and 6 accurately provided recurrence rates. There was significant heterogeneity among the groups, with I2 = 54%. A random effects model (REM) was needed for the analysis. The data proved that the recurrence rate between the TEM and the ESD was p > 0.05 (OR = 1.23, 95% CI = 0.56–2.72, p = 0.60), as shown in Figure 2.
R0 resection
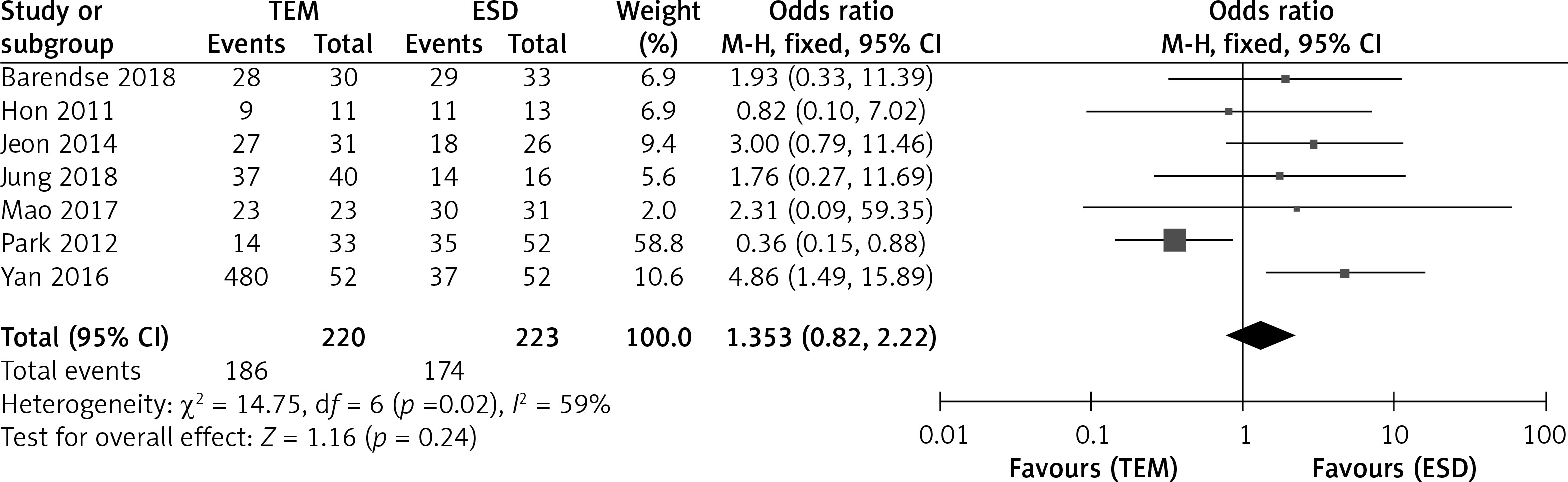
Out of 10 literature reports, 7 reported the R0 resection rate, and there was significant heterogeneity among the groups, with I2 = 59%. An REM needed to be utilized for analysis. This showed that the R0 resection rate between the TEM and ESD groups was p > 0.05 (OR = 1.35, 95% CI = 0.82–2.22, p = 0.24), as shown in Figure 3.
Hospital stay
Out of 10 literature reports, 7 reported hospitalization time, and there was significant heterogeneity among the groups, with I2 = 84%. An REM needed to be used. It showed that the hospitalization time of the TEM group was lower than that of the ESD group, with an inter-group comparison p < 0.05 (SD = 0.48, 95% CI = 0.26, 0.69, p < 0.001), as shown in Figure 4.

Perforation
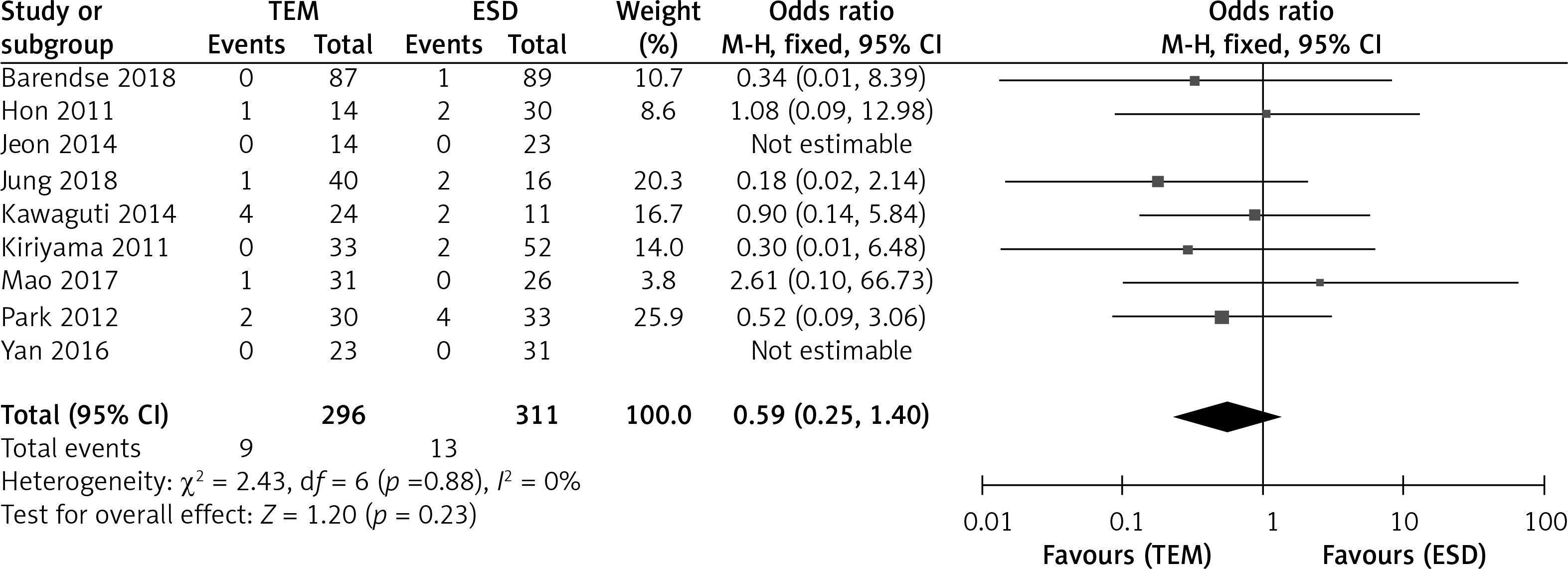
Out of 10 literature reports, 9 reported the incidence of perforation in patients, and there was no significant heterogeneity between groups. I2 = 0%, and an FEM needed to be used. The results demonstrated that there was no statistically significant difference in the perforation incidence between the two groups (OR = 0.59, 95% CI = 0.25–1.40, p = 0.23), as shown in Figure 5.
Bleeding
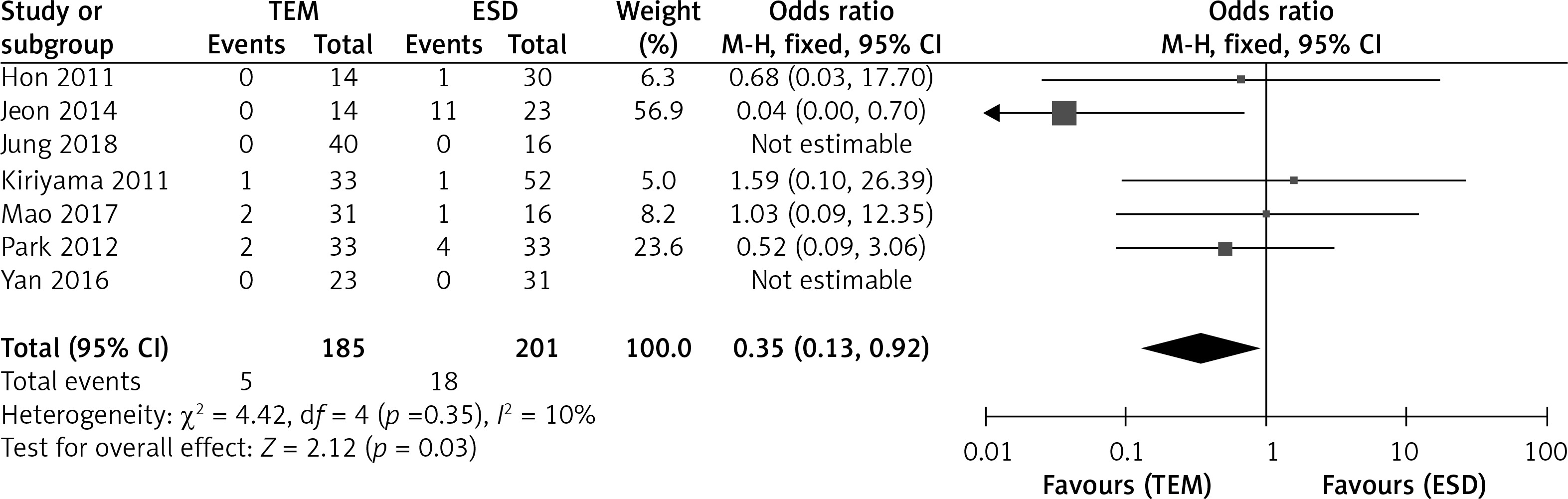
Out of 10 literature reports, 7 reported the incidence of puncture bleeding in patients, with no significant heterogeneity between groups, and I2 = 10%. An FEM needed to be utilized. This showed that the bleeding incidence in the TEM was significantly lower (OR = 0.35, 95% CI: 0.13–0.92, p = 0.03), as presented in Figure 6.
Sensitivity analysis
Sensitivity analysis was conducted on each indicator, and after removing each original study one by one, no significant changes were observed in all results, indicating the robustness of the results obtained in this study.
Publication bias analysis
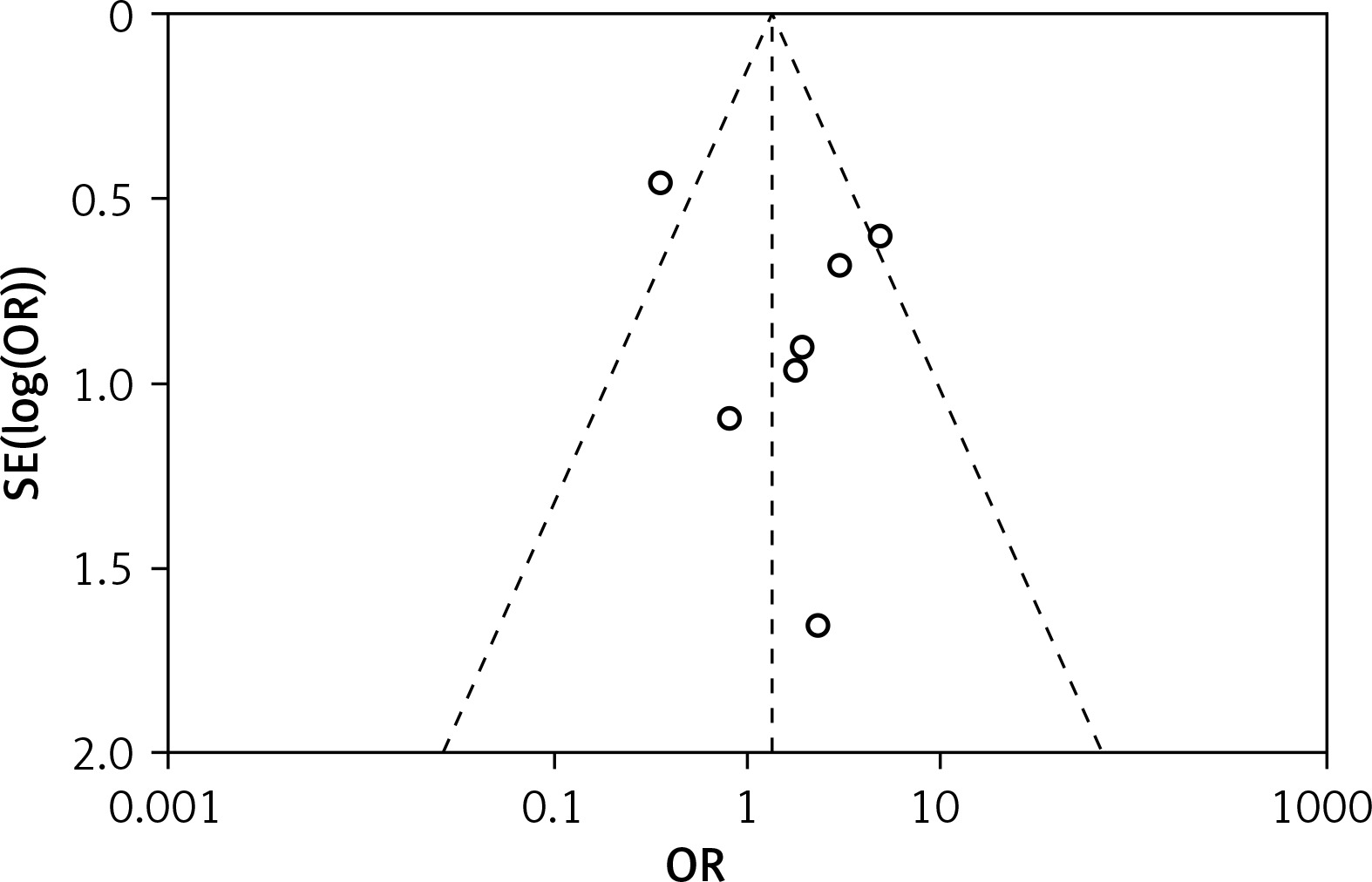
We constructed a funnel plot with recurrence rate as an indicator. The results showed that most of the scatter points in the study were within the 95% CI, indicating a certain degree of data bias in this study, but the likelihood was relatively small. The results are presented in Figure 7.
Discussion
Rectal tumors are common malignant tumors of the digestive system, seriously threatening the wellbeing and health of people. The pathological characteristics of rectal tumors are still unclear [15]. The global incidence rate of colorectal cancer among young people is rising, and it is currently the 3rd leading cause of cancer death within people under 50 years of age [16]. Among them, rectal neuroendocrine tumor is a rare colorectal tumor, and its prevalence rate has increased 10 times since it was accidentally found in the era of colorectal screening [17]. It can be seen that clinical research on the treatment of rectal tumors is an important direction. With the development of early screening technology, the recognition rate of early patients has improved. Endoscopic therapy technology is extensively adopted in the diagnosis and treatment of colorectal tumors because of its advantages of minimal trauma and good healing. Early rectal tumors can usually be treated through local resection [18]. TEM and ESD are the two main types of endoscopic local resection, each with its own advantages.
TEM technology adopts transanal endoscopic resection of tumors, which has small trauma and low bleeding risk, but it is difficult to operate and has a long learning curve. TEM can be used for endoscopic resection of highly suspicious deep submucosal infiltrating T1 rectal cancer, and has become a feasible alternative to endoscopic treatment such as submucosal resection or intermuscular dissection resection [19]. In the treatment of early rectal cancer, TEM technology provides an alternative to radical surgery of total mesorectal excision, which can reduce the occurrence of adverse events without affecting the treatment results [20]. ESD technology uses endoscopic layer-by-layer dissection to remove tumors, which is simpler than TEM, but has a higher risk of intraoperative bleeding and perforation. Takeuchi’s study [21] found that endoscopic closure of mucosal defects after ESD can decrease the risk of postoperative adverse events, but achieving complete closure for larger mucosal defects is relatively difficult. Both techniques can achieve a high R0 resection rate and a lower risk of tumor recurrence, and are widely used in curing early colorectal tumors.
This manuscript systematically evaluated the clinical effect and safety of TEM and ESD endoscopic therapy techniques in the treatment of colorectal tumors using the meta-analysis method for the first time. The results showed that the two techniques had similar effects in achieving a high R0 resection rate and low risk of tumor recurrence. However, TEM technology is superior to ESD technology in shortening hospital stay and reducing postoperative bleeding risk, and the risk of postoperative perforation is comparable between the two technologies. Therefore, TEM is more surgically safe than ESD. The research results are consistent with previous reports, confirming the advantages of TEM and ESD in the treatment of colorectal tumors. However, this study also has certain limitations, such as a limited number of included studies and relatively low quality of some papers, which can affect the precision of the research outcomes. Meanwhile, the research designs are all retrospective studies, which cannot completely avoid the impact of selection and testing bias. Meta-analysis cannot solve the problem of heterogeneity between studies, which can have an impact on the results’ reliability. Hence, the conclusions of this manuscript need to be verified by a higher quality prospective cohort study. Future research can choose a multicenter prospective randomized controlled study design, expand sample size, and strictly control study quality to generate higher-level evidence. In addition, other clinical related outcome indicators such as surgical difficulty and economic indicators should be considered for a more comprehensive and objective evaluation of the two technologies.
Conclusions
Both TEM and ESD endoscopic treatment techniques can achieve a higher R0 resection rate and lower tumor recurrence risk in the treatment of colorectal tumors. However, TEM technology may have higher surgical safety than ESD technology, and can shorten postoperative hospitalization time and lower postoperative bleeding rate.