









Introduction
In addition to the elevated mortality rate, hepatitis C (HC, a hepatotropic RNA virus that induces progressive damage of liver tissues) is one of the causes of hepatic cirrhosis and hepatocellular carcinoma. Egypt exhibits the highest prevalence of HC globally, with an estimated rate of 32% among middle-aged Egyptian men [1]. One of the most frequent conditions that impair the quality of life of HC men is erectile dysfunction (ED) [2]. The condition of insufficient penile erection for successful vaginal penetration/intercourse and adequate sexual performance is referred to as ED. In HC-positive men, the reported prevalence of ED is 39% [3]. It is unclear exactly how chronic HC results in ED [4].
A theoretical pathway dependent on inflammation is one explanation. The development of ED may be impacted by a variety of HC-induced cytokines, which results in chronic systemic inflammation, elevated oxidative stress, insulin resistance syndrome, endothelial dysfunction, and apoptosis [5].
Deficient synthesis of proteins, in particular plasma albumin, is another suggested explanation for ED development in men with HC-decompensated liver cirrhosis. Decreased albumin synthesis lowers the response of penile tissues to testosterone, hence the sexual desire and sleep-associated penile erection decrease [4].
Neuropsychological disturbances/symptoms described in the absence of HC-decompensated liver cirrhosis [6] may aggravate ED symptoms in HC men [7]. Men with HC may experience vague symptoms such as asthenia, agitation, general malaise, muscular and articular pains, and headaches. Most of the time, these symptoms do not require medical attention, but they can influence the patient’s perception of physical well-being and lead to depression, sadness, anxiety [8], mood disturbances [9], low self-esteem [10], and ED [5, 7].
Exercise is a simple, safe, and affordable solution that can be taught to anyone. In several chronic illnesses, physical activity is crucial for maintaining and enhancing physical, psychological, and sexual health [11–13]. The proposed benefits of exercise have some support in HC [1, 14] and ED studies [15, 16]; however, further research is needed to explore these benefits in HC men with ED.
Aim
To decrease its detrimental effect on psychological well-being, quality of life, and intimate relationships, HC-associated sexual impairment should be continuously screened and treated in men [7]. Because the role of exercise in ameliorating the psychological burden associated with ED in HC men was not explored, this research aimed to do this.
Material and methods
Ethics
Consent was obtained from all HC men, and Declaration of Helsinki ethical standards were strictly followed by the authors of this HC study. The institutional (Cairo University) approval reference of this HC study is P.T.REC/012/004114.
Settings
Men in this HC study were recruited from El-Sahel Teaching Hospital (andrology outpatient clinic). The period of recruitment was 5 months (from 15 October 2022 to 15 April 2023).
Inclusion criteria of HC men
Men were included if they were married, their body mass index was < 30 kg/m2 (to exclude the negative effects of obesity on penile erectile functions). Hepatitis-C-positive men were included if they complained of ED > 6 months. Mild-to-moderate ED patients were selected. ED diagnosis was based on achieving a score equal to 21-8 on the popular for-diagnosing ED questionnaire, the Arabic-Version of the Five-Item Version International Index of Erectile Function (IIEF-5). The mean ± SD of the age of the included men was 41.32 ±6.74 years.
Exclusion criteria of HC men
A gastroenterologist screened HC men to exclude cases of hepatic cirrhosis or carcinoma, other forms of hepatitis, hypertension, cardiovascular diseases (e.g. metabolic syndrome), other liver diseases (e.g. fatty liver). If the same physician reported the participant was free from respiratory, systemic (diabetes), renal, autoimmune, and neuropathic disorders, the participant was included.
An andrologist screened HC men to exclude cases of prostatic disorders, hypogonadism, or penile shaft problems/implants. Men were excluded if they had been administered pharmacotherapies for ED. Men with musculoskeletal disorders (lower-limb arthritis or severe lumbar spine disease etc.) were also excluded.
HC men were excluded if they had known psychological or mood disorders and were receiving pharmacotherapies for depression, mood stabilization, and psychotic disorders. HC men were also excluded if they were unmarried, smokers, or homeless. Men who used drugs/alcohol or were co-infected with HC and human-immunodeficiency virus were also excluded.
Randomization of HC men
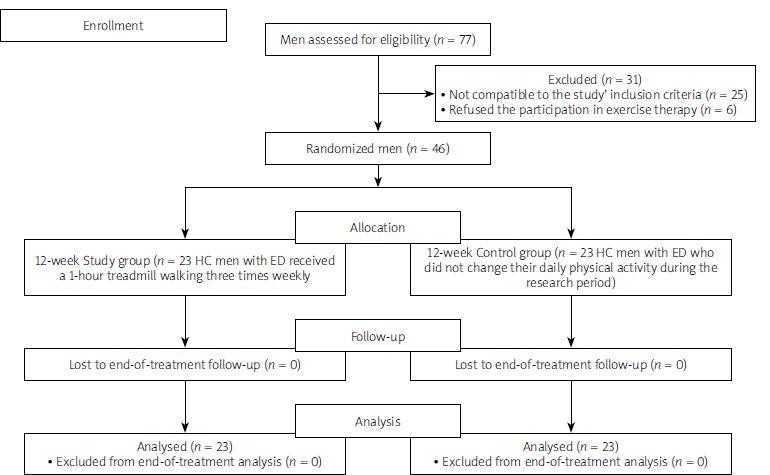
A computerized randomized HC-patient block list randomly assigned men to a walking exercise group (WEG, n = 23) or non-exercise control group (NECG, n = 23) (Figure 1). To decrease the bias of results, randomization was done by a physiotherapist blinded to the details of this HC study.
Protocol of the walking program
The HC participants allocated to WEG attended a local physiotherapy centre 3 times per week for 12 weeks to perform the walking program under the supervision of a licensed physiotherapist. At 40–60% of the maximal heart rate (HR(max)), all HC participants were advised to start and end the walking protocol with a cardiovascular warm-up and cool-down (a 5-minute treadmill walk for each). At 60–75% of HR(max), the main goal for every HC participant was to perform a 150-minute, moderate-intensity treadmill walking in the week (each session lasted 50 min).
Outcomes
IIEF-5
Each HC man received an Arabic-language printed copy of the IIEF-5 to fill in both before and after the 12-week walking protocol. The extracted mild, mild-to-moderate, moderate, and severe ED scores from IIEF-5 were classified as follows: 17 to 21, 12 to 16, 8 to 11, and 1 to 7, respectively. A score of 22 to 25 is referred to as a normal erectile function [16]. IIEF-5 was the primary outcome of this HC study.
Psychological measures
Ten-statement Rosenberg self-esteem scale
The general sense of self-worth/self-acceptance was measured in HC men by the ten-statement Rosenberg self-esteem scale (TSRSE). The ten statements of the scale are designed to be both positive and negative in equal measure [17]. The total-score range of TSRSE is between 0 and 30. In order to calculate the total score of TSRSES, the 3rd, 5th, 8th, 9th, and 10th statements are reverse coded as follows: 0 means strongly agree, 1 means agree, 2 means disagree, and 3 means strongly disagree, while the 1st, 2nd, 4th, 6th, and 7th statements were coded as follows: 3 means strongly agree, 2 means agree, 1 means disagree, and 0 means strongly disagree. Finally, the score of all 10 statements are summed to determine the final score of TSRSE. Scores ranging from 15 to 25 are within normal-range self-esteem, scores > 25 imply high self-esteem, while scores < 15 imply low self-esteem [18].
Profile of mood states
The Profile of Mood States Questionnaire (POMSQ) is a survey of mood states/disturbances. On a 5-point scale ranging from “not at all = 0” to “very = 4”, HC men rated 65 adjectives of POMSQ based on how strongly they had felt/sensed each one in the previous 7 days. Six overall scores of POMSQ (tension, despair, anger, weariness, bewilderment, and vigour) are summarized from the results of the 65 adjectives (7 of 65 adjectives are dummy adjectives that were ignored from the calculation). Scores – ‘’tension, despair, anger, weariness, and bewilderment’’ - were summed, then the result was subtracted from the vigour score to obtain the total score of mood disturbance. Lower scores of POMSQ were a sign of more stable mood profiles [19] in the tested HC men.
Beck Depression Inventory
To supply a quantitative evaluation of the severity of depression, Aaron T. Beck developed the Beck Depression Inventory (BDI) (a self-report inventory with 21 questions and numerous answers). Each question of the BDI has a score range from 0 to 3. Higher BDI scores are associated with more depression symptoms [20].
The required sample size of men with ED and HC
From an 80%-power sample size test (Power G program, effect size 0.8, primary-outcome IIEF-5 variable), the required number of ED-associated HCV participants to accomplish this trial was 20 men in each group (a statistician calculated these results from the data of a 16-patient exercise-therapy pilot test). To eliminate the drop-out effect (estimated at 15%) on the final results, 3 men were added to every HC group.
Statistical analysis
The used statistical tests in this HC study were the unpaired and ANOVA (repeated measure) tests. The first test was used to compare the demographic (HC men’s ages and body mass indices) and clinical (albumin, total bilirubin, prothrombin, and international normalized ratio) data between groups, and the second one was used to compare the results (outcomes) among and within groups. The 2 tests were used after the confirmation of the SPSS statistical test (Kolmogorov-Smirnov test) that the results were normally distributed.
Results
Before starting the walking program there was no significant between-group pre-treatment difference regarding clinical data (albumin, total bilirubin, prothrombin, and international normalized ratio), demographic data (age and body mass index (as shown in Table I)), or outcomes (POMSQ, BDI, AST, IIEF-5, ALT, and TSRSE (as shown in Table II)). After finishing the 12-week walking program, as shown in Table II, the within-group comparison showed significant improvements in POMSQ, BDI, AST, IIEF-5, ALT, and TSRSE in WEG only. The post-outcome comparison between WEG and NECG showed significant improvements in POMSQ, BDI, AST, IIEF-5, ALT, and TSRSE in favour of WEG.
Table I
Pre-treatment data in HC groups
Table II
Results of HC study outcomes
Discussion
There has been limited investigation of the effect of regular exercise on the psychological burden, liver enzymes, and HC-associated ED in HC men, so this study is the first one handled this topic to document significant improvements in POMSQ, BDI, AST, IIEF-5, ALT, and TSRSE after 12-week treadmill walking program in HC men with ED.
In long-standing chronic infectious diseases, exercise – via cardiovascular risk reduction, respiratory/functional complications enhancement, quality of life improvement, pain tolerance improvement, and immunity strengthening – improves ED and ED-associated psychological burden [12]. Considering the constant fear among the majority of liver-disease men of taking pharmacotherapies for associated diseases/dysfunctions, including ED, utilizing exercise to improve sexual dysfunction and its related psychological burden is warranted. Exercise-induced improvements in physical functions and ED could improve ED-associated depression, low self-esteem, and mood disturbances.
It was believed that when a man successfully completes/achieves a relatively difficult job (such as a long-term structured exercise program), his self-image, self-concept, competence, self-worth emotions, ability to handle daily life stressors, and social-cognitive interaction are enhanced [21]. This would then improve psychological states like decreased despair, depression, and bad mood. These suggestions are compatible with exercise-induced biochemical cerebral changes that affect mood and depression due to increased happiness-mediator products such as endorphin, serotonin, and norepinephrine [22].
Besides the above-mentioned (bio)psychological aspects of exercise that may improve ED-associated psychological burden, it is postulated that regular walking can improve ED by increasing penile blood flow. This occurs through increasing vasodilating substances (such as nitric oxide), relaxing smooth muscles of penile (pudendal) vessels, decreasing pro-inflammatory markers, correcting long-term atherosclerotic risk factors, and inducing vascular biochemical/hormonal changes. Perceived improvement in general physical fitness, depression symptoms, low self-esteem symptoms, and mood disturbances after regular walking training can improve ED [16, 23, 24] in HC men.
HC patients show inhibited proliferation of hepatic stellate cells, improved immune system/activity, increased production of anti-inflammatory biomarkers, increased fighting/resistance against further infection/inflammation of new hepatocytes, and decreased the chances of new HC viral replications after long-term exercise. This not only explains the reported improvements in WEG’s ALT and AST but also promises to return the normal functioning of hepatic tissue to be able to face, limit, or prevent HC-induced extra-hepatic complications [25], including ED.
The reported decrease of HC patients’ liver enzymes (ALT and AST) in previous studies that used the 3-month [1] or 2-month [25] treadmill walking provided support for the reported improvement of liver enzymes in the WEG.
Two Nigerian studies showed a significant IIEF improvement due to C-reactive protein improvement after using a noninvasive/non-pharmacologic treatment, 8-week interval [23], or continuous [24] treadmill walking in hypertensive males with ED, supporting the reported IIEF-5 improvement in the WEG.
In an Italian study, 209 men (body mass index > 30 kg/m2) were divided into 2 groups at random: an intervention group (n = 104, of whom 34% had normal erections) and a control group (n = 105, of whom 36% had normal erections). While the second group received basic, uninform information, the first group received precise advice about losing body mass and exercising more. The 2-year follow-up of men’s erectile function revealed that both the intervention (56%) and control (38%) groups noticed an increase in normal erections [26]. Through exercising more and eating less, the 2-year follow-up of IIEF-5 in another Italian study in obese men with ED showed significant improvement after a 10% weight reduction [27].
Cycling as a cardiac rehabilitation program significantly improved the ED in ischaemic heart disease men [28], providing additional support for the reported IIEF-5 improvement in the WEG. Two months of exercise training plus pharmacological therapies produced greater improvement in ED than pharmacological therapies alone in men with cardiovascular risk factors such as metabolic syndrome [29] and obesity [16].
As support for the important role of exercise in alleviating the psychological burden in HC patients, our choice of lifestyle modification to improve the psychological burden in HC patients was supported by another pilot study that recommended the use of regular physical activity to improve the psychological aspects in HC patients [14]. Improved BDI of HC men in the present study was supported by the BDI of major depression [30] or diabetic patients [31], which was significantly improved after long-term aerobic exercise (walking program). Also, older participants’ self-esteem and depression (assessed via BDI) improved after participation in 16 weeks of training.
A comparison using the depression scale and short-form POMSQ between a 12-week exercised preadolescent group and a non-trained preadolescent group showed significant improvement in favour of the first group [22]. Also, 52 asymptomatic sedentary women who underwent a 10-week aerobic and resistance training program showed a significant POMSQ, supporting our results [32]. In healthy young participants, 30 min of aerobic exercise significantly improved their mood (assessed via the POMSQ) [33, 34].
Regarding our improved TSRSE results, physical exercise (16-week weight training) significantly improved the TSRSE of 27 young college students [35]. Also, in elderly residents in a nursing home [36] and in women with fibromyalgia [37], a 1-month exercise program significantly improved their TSRSE [36, 37].
However, in a study containing 375 insulin-resistant old people with ED divided into 2 groups (group A, which received 175 min of physical activity per week to reduce their body mass index over a 1-year follow-up regime, and a control group which received general support/education about insulin resistance disease), the irreversible erection-related neurogenic/vascular abnormalities in insulin-resistant subjects explained the poorer penile erection that occurred in the exercised elders as compared to the control non-exercised ones [38].
The role of long-term physical activity (applied regularly for weeks) in preventing cardiovascular risk factors, insulin resistance, and obesity, in liver illnesses, is further supported by its ability to induce significant improvement in liver enzymes in middle-aged [39] and older patients [40]. A 10-week relaxation and aerobic exercise program did not affect the BDI of fibromyalgia patients, contradicting our results [41]. The after-exercise 1-day assessment of POMSQ did not show significant changes, but this may be due to the application of one exercise session in the assessed women [42]. Also, the non-significant TSRSE improvement in women who underwent 12 weeks of aerobic exercise opposed our results, possibly due to the small number of women (n = 10) [43].
Long-term follow-up to the significant improvements of POMSQ, BDI, AST, IIEF-5, ALT, and TSRSE in WEG was the main limitation to our study, which must be rectified in future studies on HC men with ED.