






This case reported a 44-year-old woman who underwent multiple interventions to the left anterior descending artery with myocardial bridging. Coronary computed tomography, myocardial perfusion imaging, and coronary angiography with intravascular imaging were performed to delineate the exact pathology.
A female patient, aged 44 years, who had undergone recurrent percutaneous coronary intervention (PCI) for the left anterior descending artery (LAD), presented with persistent angina symptoms (Canadian Cardiovascular Society Angina Grade III). She had a medical record of diabetes and hypertension. The patient received PCI treatment for LAD stenosis 1 year ago and underwent percutaneous transluminal angioplasty 10 months after the initial procedure. During the initial medical intervention, a 3.0 × 25 mm drug-eluting stent (Cre8, Alvimedica) was successfully implanted to the stenosis in the LAD artery (Figures 1 A–E). After 10 months, the patient had a second coronary angiogram (CA), and in-stent restenosis was treated with non-compliant balloon angioplasty (3.5 × 20 mm) (Figures 1 F–H). The procedures, as mentioned earlier, were conducted at a separate cardiology clinic. However, the patient was subsequently referred to our outpatient clinic with increased angina, which persisted even after minimal physical activity despite having undergone intensive medical treatment. In the index procedure, partial systolic compression was seen, and extension of the LAD looked intramyocardial. Myocardial perfusion scintigraphy (MPS) and coronary computed tomography angiography (CCTA) were performed. MPS showed severe ischaemia of the apical, anterior, anteroseptal, and anterolateral segments of the myocardium (Figure 2 A). CCTA revealed that the stent was firmly attached to the myocardium at the centre. However, there was some degree of in-stent restenosis, causing it to become slightly narrowed and resemble a cockboat (Figures 2 B–D). CA (Figure 2 E) was repeated with the guidance of intravascular ultrasound (IVUS) (Eagle Eye Platinum Digital IVUS catheter, Philips). IVUS identified the absence of metallic stent struts in the middle part of the stent and neointimal hyperplasia, leading to a diagnosis of stent fracture (Figures 2 G, H). IVUS also showed a well-expanded stent at the distal part (Figure 2 E). Due to the extensive ischaemic area on MPS imaging and the patient’s severe angina, despite the maximal medical treatment, the heart team recommended coronary artery bypass grafting (CABG). The procedure involved grafting the left internal mammary artery to the LAD, resulting in successful patient recovery. The patient was well during the follow-up, with no angina, and she also underwent MPS imaging without ischaemia.
Figure 1
Right cranial oblique view (A) and anteroposterior cranial view (B) of coronary angiography showing myocardial bridging and stenosis of left anterior descending artery (LAD). C, D – Stenting of LAD with 3.0 × 25 mm drug-eluting stent. E – Coronary angiogram (CA) showing acceptable results after stenting. F – Ten months later, after stenting, CA showed in-stent stenosis and kinking of the stent G – Percutaneous transluminal angioplasty of LAD with a non-compliant balloon (3.5 × 20 mm). H – TIMI -III flow after percutaneous transluminal coronary angioplasty (PTCA) of LAD stent
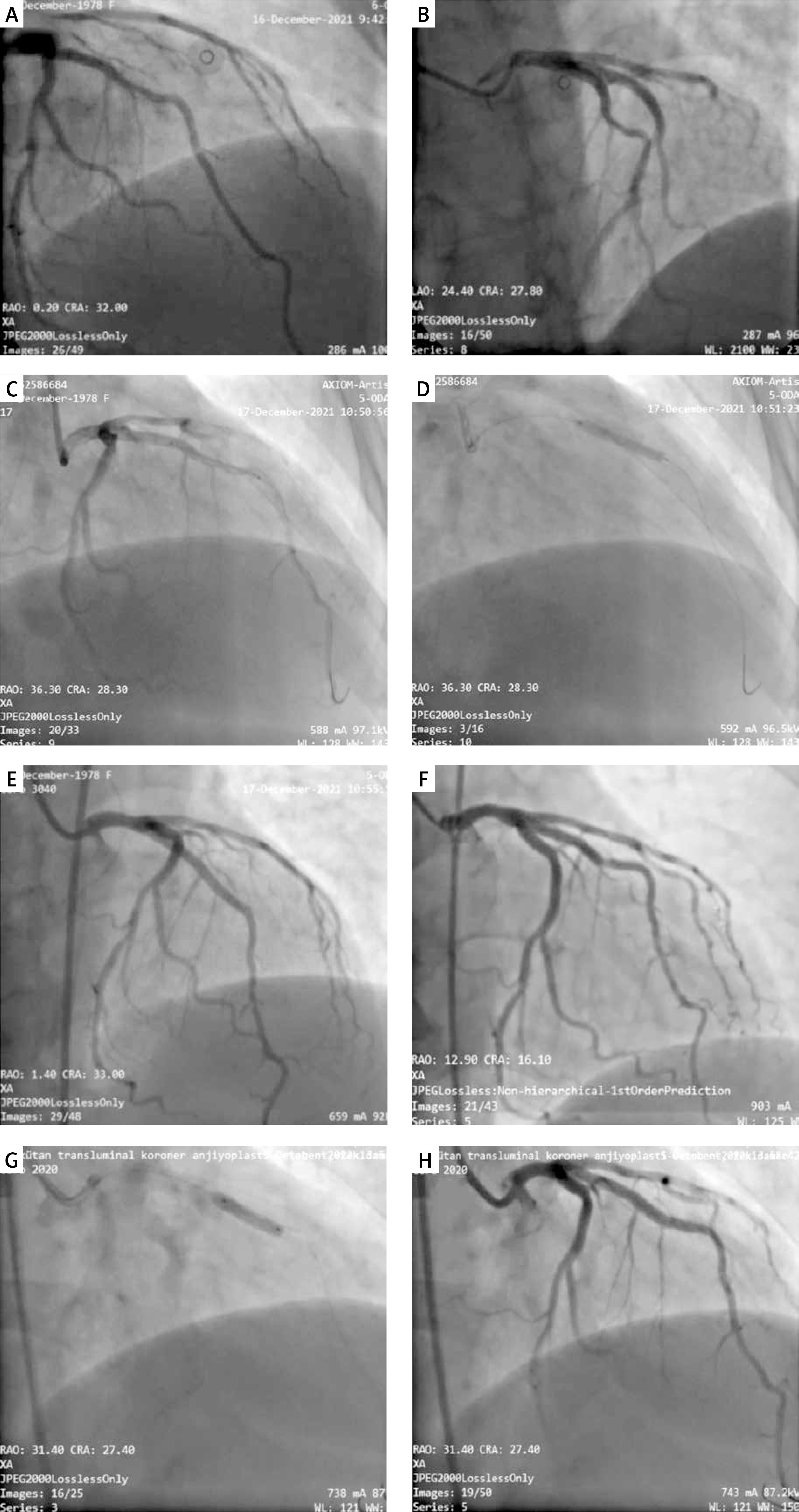
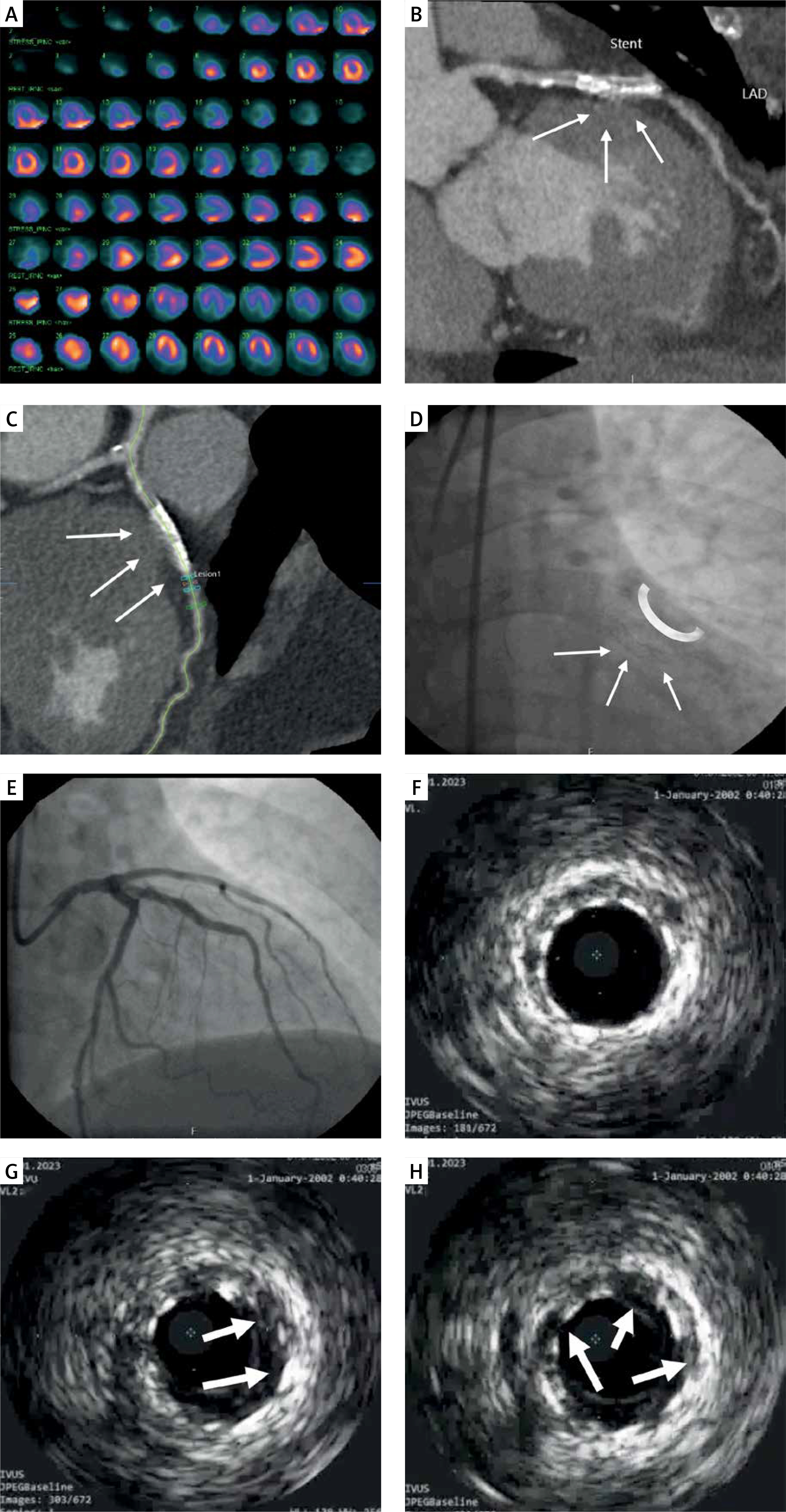
Figure 2
A – Myocardial perfusion imaging showing myocardial ischaemia of apical, anterior, anteroseptal, and anterolateral segments. B – Coronary computed tomography angiography (CCTA) shows that the stent was attaching the myocardium at the centre and became like a cockboat with some degree of in-stent restenosis. The epicardial layer was not seen in the middle part of the attached stent C – Coronary computed tomography angiography (CCTA) shows that the stent was attaching the myocardium at the centre and became like a cockboat with some degree of in-stent restenosis. The epicardial layer was not seen in the middle part of the attached stent. D, E – Coronary angiography (3rd) shows a fractured stent with good flow. F – Intravascular ultrasound (IVUS) showed a well-expanded distal part of the stent. G, H – IVUS showed a local absence of metallic stent struts and neointimal hyperplasia
Myocardial bridging is rarely associated with atherosclerosis and is mostly found in the proximal part of the bridging segment. Due to the milking effect and forceful myocardial contraction, stent fracture can occur after stenting of MB [1]. In this case, the intramyocardial segment was more profound at the middle site of the stent and resembled a half-moon sign, as previously shown by Yamada et al. [2, 3]. In this case, the stent became like a cockboat due to the forceful effect of the myocardium in the middle part. Although a greater minimal lumen area was measured in the IVUS imaging, MPS showed extended ischaemia in the anterolateral segments.
Treatment for myocardial bridge in symptomatic patients remains controversial. For patients who are unresponsive to medication, surgical interventions such as CABG and myotomy may be performed [1]. Atherosclerosis at the bridge point can add more challenges to selecting a treatment modality. CABG is an effective treatment of myocardial bridges for long-term patency; however, it cannot cure bridge segment [1]. Stenting could result in conflicting results with early occlusion and fracture of the stent [4–7]. Haager et al. reported 11 patients with mid-LAD myocardial bridging with ischaemia by perfusion imaging. They obtained good immediate angiographic results in all patients. However, target vessel revascularisation at 7 weeks was 36%, with a 45% incidence of in-stent restenosis [6]. Long-standing and cyclic mechanical stress may lead to increased shear stress, metal fatigue, and eventually stenosis and fracture [8].
Although MB is thought to have ischaemia in the heart only in the systolic phase, Rouleau et al. showed a diastolic lag time following transient systolic compression of the coronary artery in their animal study, leading to the conclusion that diastolic flow [9]. Several management options for stent fracture in this patient, including observation, the use of the stent-in-stent technique, and surgical correction, have been discussed. Due to the sizeable ischaemic area and atherosclerosis at the site of bridging, bypass graft surgery was performed.