






Introduction
The widespread concern for health issues in the late 1900s was associated with the development of health psychology [1, 2]. According to the definition formulated first by the World Health Organization in 1948, health is a state of complete physical, mental, and social wellbeing, and not merely the absence of disease or infirmity. In subsequent definitions health was regarded as a disposition or resource enabling task fulfilment or self-realization [3], as a process [4, 5], and as a function of creative coping with stress [6].
The development of systems theory with the assumption of autonomy of particular systems has led to the holistic-functional model of health, where man, located in the centre of the universe, is the subject as well as the creator of so defined health [3]. The individual is affected both by the biosphere and the sociosphere, or culture. In this approach, health is regarded not only as the absence of symptoms of disease (so-called objective health), but also as a sense of wellbeing (i.e. subjective health) that has stronger regulative power to determine human behaviour and functioning [7]. Health seen from the salutogenic perspective [5] is a process of maintaining equilibrium between environmental demands (stressors, pathogens) and the individual’s capacities (resources, potential). As a process it can be represented on a single continuum stretching from full health to disease, which allows us to distinguish various levels of human health.
Leukaemia, one of the most malignant neoplastic diseases of the blood, (of still unknown aetiology and – until recently – incurable), is particularly stressful to the patient. The stress of leukaemia is enhanced by negative and anxiety-laden attitudes that predominate in the social perception of neoplastic diseases. People suffering from cancer are frequently regarded by the public as those marked by fate, with their life prospects predetermined by the stereotype implying that cancer equals death [8]. A study on social perception of cancer 40 years later [9] revealed no particularly novel findings in this respect. Psychosomatic research sought also to identify psychological and social determinants of neoplastic diseases, as well as ways of their treatment [10].
The first Polish studies involving leukaemia patients and representing a somatopsychic approach have been conducted by the present author at the Haematology Clinic in Cracow under the supervision of Professor Julian Aleksandrowicz since the mid-1990s. The research findings point to a significant role of leukaemia patients’ self-concept in their coping with the disease [11–14]. Modern methods of leukaemia treatment, i.e. bone marrow transplantation (BMT) and haemopoietic stem cell transplantation, introduced due to the progress in medicine and related disciplines, have contributed to a change in the public image of leukaemia, from that of a lethal risk into a curable condition, challenging the patient to engage in recovery-oriented activities. Since the Bone Marrow Transplantation Unit establishment in 1998 at the Professor Julian Aleksandrowicz Haematology Clinic, Jagiellonian University Collegium Medicum, more than 1000 transplantations have been performed there in leukaemia patients over 20 years [15].
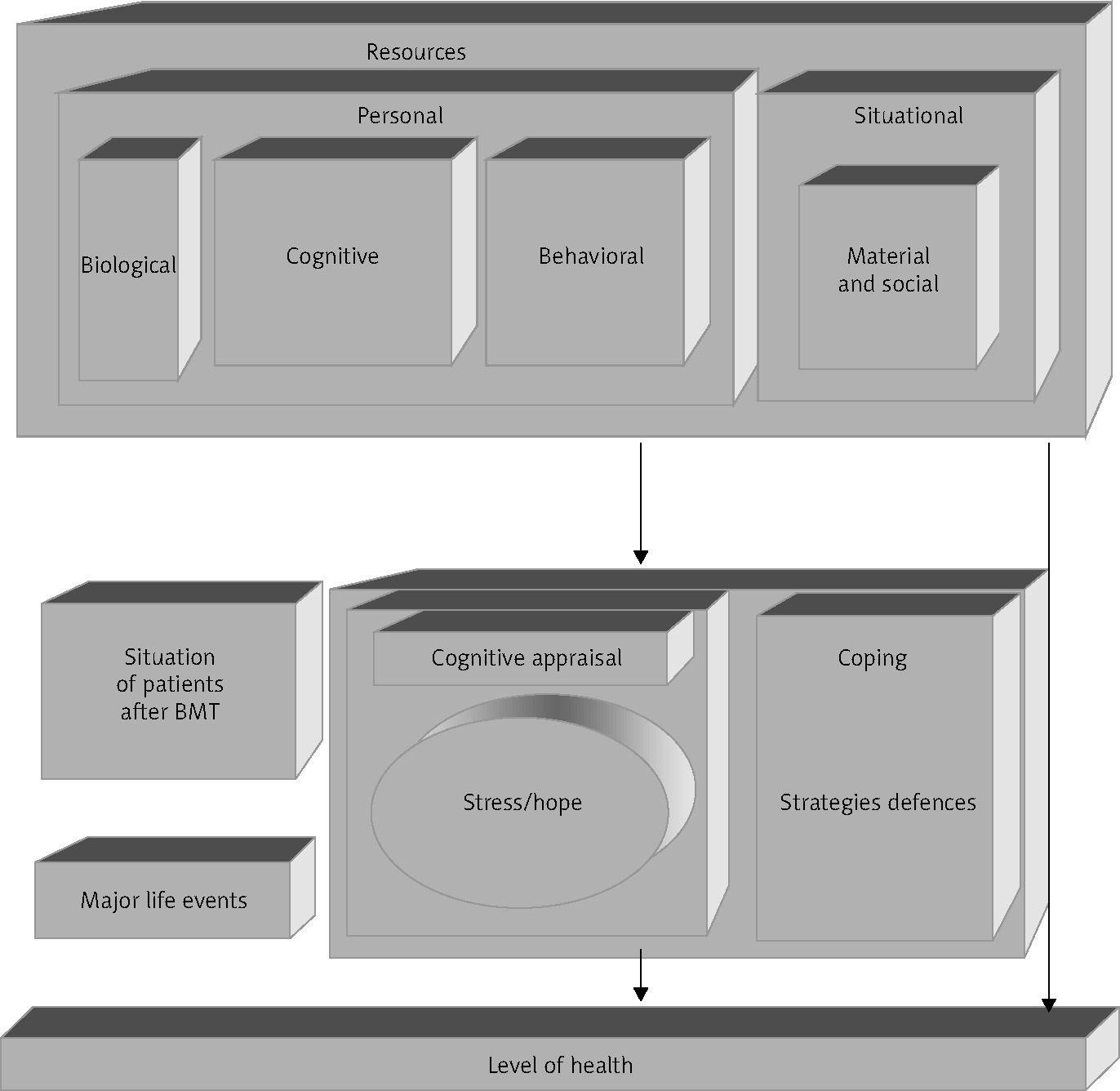
On the grounds of the Lazarus and Folkman stress theory [16], the conservation of resources theory by Hobfoll [17], the salutogenic concept by Antonovsky [5], and the present author’s clinical experiences and research involving leukaemia patients [11–14], the functional model of health (FMH) was developed and then empirically verified in a study involving healthy volunteers [6].
An important role is attributed in the FMH to personal resources including a strong sense of coherence (SOC), sense of control, and positive self-esteem jointly constituting a pro-health personality. The cited research indicates that a pro-health personality considerably enhances effective or creative coping with stress, at the same time just as strongly buffering negative stress effects (path coefficients, respectively, 0.63 and –0.63), thus acting on behalf of health [6]. The functional model of health provided a theoretical framework for the author’s research involving leukaemia patients after BMT (Fig. 1).
Furthermore, the FMH predicts that health as a function of creative coping with stress should depend on the patients’ personality dispositions, i.e. on relatively stable factors such as personal resources or styles of coping (task-oriented, emotion-oriented, and avoidant) [18]. A particularly health-promoting role in stress transactions is fulfilled by the SOC [6, 19] and by self-esteem [6, 11, 14, 20–23]. Sense of coherence, involving both cognitive and emotional factors, is most important in coping with stress, because the nature of problems is always dual: not only understanding of the problem is required, but also emotion regulation [5].
A similar role is fulfilled by the self-concept defined as a set of descriptive and evaluative beliefs about oneself. Self-esteem was found to serve a regulatory function as regards personal resources, at the same time motivating and mobilizing individuals to undertake activities that might restore their lost psychological balance, or mental health.
Based on the FMH, the following hypotheses were formulated for the study:
Material and methods
Participants in the study comprised 141 patients (61 wo-men and 80 men) after BMT performed at the Haematology Clinic, Jagiellonian University Collegium Medicum. They were examined during their check-up visits at the clinic. Most of the participants were in the age range between 20 and 40 years, and most had secondary education.
The key method used in the study was a standardized interview concerning the experience of illness and related emotions. Health was operationalized by 3 indicators: the sense of health, the sense of calmness, and the absence of anxiety. Each of the 3 indicators was self-assessed on a 10-point rating scale ranging 1–10. Each respondent was asked to rate the degree to which he or she was feeling ill/healthy and to justify his/her choice marked on the scale. The patient’s objective health assessment based on medical parameters was performed by a physician-haematologist using a similar scale. In statistical analyses the subjective health was operationalized as an aggregate mean score for the sense of health and the sense of calmness scales (ranging 1–10). Correlation between the means was sufficiently strong (r = 0.51) to calculate a global index of subjective health.
The patient’s stress level (version X1) and anxious personality (version X2) was assessed using the STAI by Spielberger et al. in the Polish adaptation (ISCL) by Sosnowski et al. [24]. Coping styles were measured with the CISS inventory by Endler et al. [25]. Personal resources including SOC and self-esteem were evaluated using, respectively, the SOC-29 scale by Antonovsky [26] and the SES scale by Rosenberg [27].
Results
Patients’ subjective health indicators are related to stress and coping styles
The patients’ subjective health was generally high, with higher mean scores on the sense of calmness and absence of anxiety scales (7.04 and 7.14, respectively) than on that sense of health scale (“feeling healthy”) (6.69). The latter variable is related to the patients’ awareness that they need continued medical care, including regular check-ups and maintenance immunosuppressive medications, which may lead to their subjective health underestimation. The highest scores were noted as regards the patients’ objective health assessed by their attending physician (M = 7.70).
The difference between mean scores of the patients’ sense of health and their physician-rated objective health (respective means: 6.69, SD = 2.52, and 7.70, SD = 2.09) as assessed by the t-test for pairs, turned out to be significant (t = –4.59, df = 139, p < 0.001). The findings show that although the patients’ objective health after the BMT is good, they tend to view their health status as moderate, and it is on their perception that their functioning depends to a large extent. Stress and coping styles in relation to all the health indicators (Table 1).
Table 1
Pearson’s r correlation coefficients of stress and coping style with all the health indicators
Pearson’s r correlation (Table 2) coefficients show statistically significant negative associations of stress with all the health indicators under study. Strong negative correlations of stress were found with sense of calmness (r = –0.58) and the absence of anxiety (r = –0.54), i.e. the higher the stress levels, the weaker the feelings of tranquillity and thus the stronger the anxiety involving a threat to the subjective patients’ health. It should be noted that the experienced stress was unrelated to the patients’ physical health.
Table 2
Pearson’s r correlation coefficients between coping styles and personal resources
Further correlation analyses revealed strong negative associations of emotion-oriented coping with both the patients’ sense of calmness (r = –0.53, p < 0.001) and the absence of anxiety (r = –0.38, p < 0.001), as well as positive associations of avoidance coping through seeking social contacts with their sense of health (feeling healthy) (r =0.19, p < 0.05) and calmness (r =0.25, p < 0.01). In other words, the higher the patients’ tendency to employ emotion-focused coping, the lower their tranquillity or feelings of inner peace and harmony, which translates into higher anxiety levels threatening to personality integration, i.e. to their subjective health.
Coping styles are related to the patients’ personal resources
Statistically significant positive correlations (Pearson’s r) of task-oriented coping were found with self-esteem (r = 0.49, p < 0.001) and SOC (r = 0.33, p < 0.001), but negative correlation with anxious personality (r = –0.31, p < 0.001).
This affective-motivational component of SOC leads the patients to believe that life is worth fighting for and that they should strive to regain health after a bone marrow transplantation. Enhanced avoidant coping through seeking social contact was also associated with the SOC, particularly with its meaningfulness component, (r = 0.42, p < 0.001) and, at a trend level, with self-esteem (r = 0.26, p < 0.05). On the other hand, coping by seeking social contacts negatively correlated with anxious personality (r = –0.28, p < 0.001). Moreover, statistically significant but negative correlations of emotion-focused coping with SOC (r = –0.46, p < 0.001) and self-esteem (r = –0.41, p < 0.001) should be noted, while strong and positive correlations were seen with anxious personality (r = 0.67, p < 0.001).
Personality determinants of the patients’ subjective health
The stepwise regression analysis (Table 3) shows that the patients’ subjective health is directly predicted by their objective health (0.413) and stress (–0.285), counterbalanced by the sense of meaningfulness (0.244) as the affective-motivational component of SOC. The multiple correlation coefficient (R = 0.712) indicates a marked effect of the analysed set of predictors on the patients’ subjective health, while the coefficient of multiple determination r2 = 48.1% allows us to conclude that about 50% of variance in the dependent variable, i.e. in subjective of the patients’ health, is explained by the proposed model.
Table 3
Predictors of subjective health
Discussion
The aims of the study were to assess subjective health and its psychological predictors in leukaemia patients after BMT. The theoretical rationale of the study was the FMH.
Correlation analyses indicated statistically significant negative correlations of stress with all the self-rated indicators of the patients’ health. This means that the stress they experience due to their illness, transplantation, and in their daily life may be health threatening. The higher the intensity of experienced stress, the lower the patients’ self-assessed subjective health level. Further correlation analyses show that personal resources including SOC, and particularly positive self-esteem as a resource of regulatory character, are associated with the tendency to use both task-oriented coping, and avoidant coping through seeking social contact. Personal resources significantly and strongly counteract the emotion-oriented coping style considerably enhanced by an anxious personality. This regularity has been confirmed by numerous studies [6, 17–19, 22, 28].
Studies by Jabłoński et al. [29] in patients with acute leukaemia undergoing treatment have shown increased levels of their SOC, particularly of the meaningfulness component, at 4-week and 12-week follow-ups. These findings suggest that SOC corroborates the fundamental importance of this variable for recovery processes [6, 22, 26, 28].
Stepwise regression analyses revealed that the psychological dimension of the patients’ health was predicted first and foremost by their physical health and experienced stress level. Stress was buffered by personal resources such as a strong sense of meaningfulness giving a profound meaning to the patients’ lives and coping with illness, and encouraging them to actively strive for recovery.
Conclusions
Psychotherapeutic interventions should be aimed at reducing patients’ distress and anxiety. A particularly important role in buffering BMT patients’ anxiety and depression [29] is ascribed to the enhancement of their SOC and self-esteem [21, 22, 28, 30], as well as to the provision of active support to the family [31, 32], promoting the patients’ subjective health. The present study findings suggest that while contemporary medicine can save leukaemia patients’ lives owing to the BMT, the recovery of their mental and subjective health as a foundation of their good functioning depends on psychological mechanisms, the patient`s activity, and a supportive psychologist.