
Dear Editor,
Malignant hyperthermia (MH) is a rare, dominantly inherited phar-ma-cogenetic disorder triggered by halogenated anesthetics and succinylcholine, with an incidence between 1 : 10,000 and 1 : 50,000 anes-thesia cases [1, 2]. MH is caused by increased calcium influx into the sarcoplasm, leading to sustained muscular contractions and hypermetabolism [2]. MH can start immediately after exposure to anesthetics or hours later, even in the postoperative period [1, 2], with the occurrence of hyperthermia, tachycardia, hypercapnia, metabolic acidosis, muscle rigidity, rhabdomyo-lysis, tachypnea, increas-ed oxygen consumption, hyperkalemia, arrhythmias, myoglobinuria, renal failure, or disseminated intravascular coagulation (DIC) [2]. Early diagnosis and specific treatment with dantrolene sodium have decreased mortality to 11% [2].
The accurate diagnosis of MH may be challenging in some situations, such as during cardiac bypass and in patients with cervical spinal cord lesions [3, 4]. Patients with chronic kidney disease (CKD) are another group with confounding factors as they can present with metabolic acidosis, hyper-kalemia, and pulmonary edema [5]. Additionally, during organ transplantation, it is necessary to perform a differential diagnosis of post-reperfusion syndrome, characterized by abrupt hemodynamic instability, acidosis, and hyperkalemia [6].
Here, we report a suspected MH crisis in a renal transplantation recipient and present a review of cases reports of suspected MH crisis during solid organ transplants (Table 1) [7–15]. Written consent has been obtained from the patient for this publication.
TABLE 1
Case reports of MH during transplantation
| Author, year | Age (years) Sex | Transplant | Triggering anesthesia | MH onset CGS Rank | Dantrolene | Maximum CPK Myoglobin | Patient/ Graft evolution | Recrudescence | MH Investigation |
|---|---|---|---|---|---|---|---|---|---|
| Byers et al., 1987 [7] | 33 Female | Living donor kidney transplantation | Halothane | Onset: 4 h CGSc: 61 Rank: 6 | Bolus: 2.4 mg kg–1 Maintenance: new bolus 12 h after | CPK: 683 units (24 h after) | Good graft function | Not described | No |
| Simons et al., 1988 [8] | 35 Male | Living donor kidney transplantation | Isoflurane | Onset: 3 h CGSc: 76 Rank: 6 | Bolus: 3 mg kg–1 Maintenance: 1.8 mg kg–1 6/6 h for 24 h + orally for more 24 h | CPK: 862 units L–1 (36 h after) | Postoperative period uneventful | No | No |
| Striebel et al., 1991 [9] | 30 Female | Deceased donor kidney transplantation | Isoflurane | Onset: 2 h CGSc: 53 Rank: 6 | Bolus: 2 mg kg–1 Maintenance for 24 h (total: 700 mg) | CPK: 1024 units L–1 Myoglobin: 800 µg L–1 (24 h after) | Good graft function and patient well | No | In vitro contracture test positive |
| Caglar et al., 2002 [10] | 22 Male | Living donor kidney transplantation | Isoflurane | Onset: 4.5 h CGS: (impossible to calculate – missing data) Rank: 6 | Bolus: 2 mg kg–1 Maintenance: not described | CPK: 57100 units L–1 | Good graft function and patient well | Not described | No |
| Fernandes et al., 2007 [11] | 48 Male | Deceased donor hepatic transplantation | Isoflurane | Onset: 1.5 h CGS: 50 Rank: 6 | Bolus: 1 mg kg–1 Maintenance: 1 mg kg–1 8/8 h for 48 h | CPK: 3134 units L–1 (day 2) | Good graft function and patient well | Not described | No |
| Shih et al., 2010 [12] | 37 Male | Living donor hepatic transplantation | Volatile anesthetic not specified | Onset: 2 h CGS: 53 Rank: 6 | Bolus: 1.2 mg kg–1 Maintenance: no | CPK and myoglobin negatives | Good graft function and patient well | No | Not described |
| Tsujikawa et al., 2013 [13] | 51 Male | Living donor hepatic transplantation | No triggering agents used | Onset: 2.5 h CGS: (impossible to calculate – missing data) Rank: 5 | Bolus: 2.5 mg kg–1 (in ICU – 12 h after) | CPK and myoglobin “elevated” | Not described | No | Genetic test: glycine-to-adenosine substitution at Leu197 in the RYR1 gene (it doesn’t affect function of RYR1) |
| Bick et al., 2016 [14] | 33 Female | Double-lung transplantation | Sevoflurane and succinylcholine | Onset: 45 min CGSc: (impossible to calculate – missing data) Rank: 5 | Bolus: done (not specified) Maintenance: no | CPK: not described Myoglobin: 388 ng L–1 | Good graft function and patient well | No | No |
| Srinivasan et al., 2020 [15] | 5 Male | Living donor kidney transplantation | Isoflurane and sevoflurane | Onset: 5 h CGS: 61 Rank: 6 | Bolus: 1 mg kg–1 Maintenance: 0.25 mg kg–1 h–1 for 4 h | CPK: negative | Good graft function and patient well | No | No |
A 47-year-old white man (height 170 cm, weight 85 kg, BMI 29.4 kg m–2), with hypertension and end-stage CKD secondary to focal-segmental glome-rulosclerosis, was admitted to undergo unrelated living donor kidney transplantation. Previous spinal anesthesia for umbilical hernia repair was uneventful, as was general anesthesia in relatives. He presented with metabolic acidosis (pH 7.26) and mild hyperkalemia (potassium 5.4 mmol L–1). Other laboratory tests, electrocardiography, and chest radiography findings were normal. He had undergone hemodia-lysis the day before the surgery, and there was no volume loss. His daily oral medications included valsartan, amlodipine, and furosemide.
Monitoring included continuous electrocardiogram, oximetry, capno-graphy, non-invasive blood pressure, esophageal thermometer, and bladder catheter; active heating was not used. His vital signs were as follows: initial blood pressure (BP), 150 × 90 mmHg; heart rate (HR), 78 beats min–1; oxygen saturation (SatO2), 96%; and body temperature, 36oC. General anesthesia was induced with 4.0 µg kg–1 fentanyl, 2.3 mg kg–1 propofol, and 0.15 mg kg–1 cisatracurium. After orotracheal intu-bation, anesthesia was maintained with 6.5% desflurane, and the patient was mechanically ventilated with pre-ssure-controlled ventilation. The do-- nor received peridural 0.375% ropiva-caine, and general anesthesia was induced with fentanyl, propofol, and cisatracurium, and maintained with desflurane 6%.
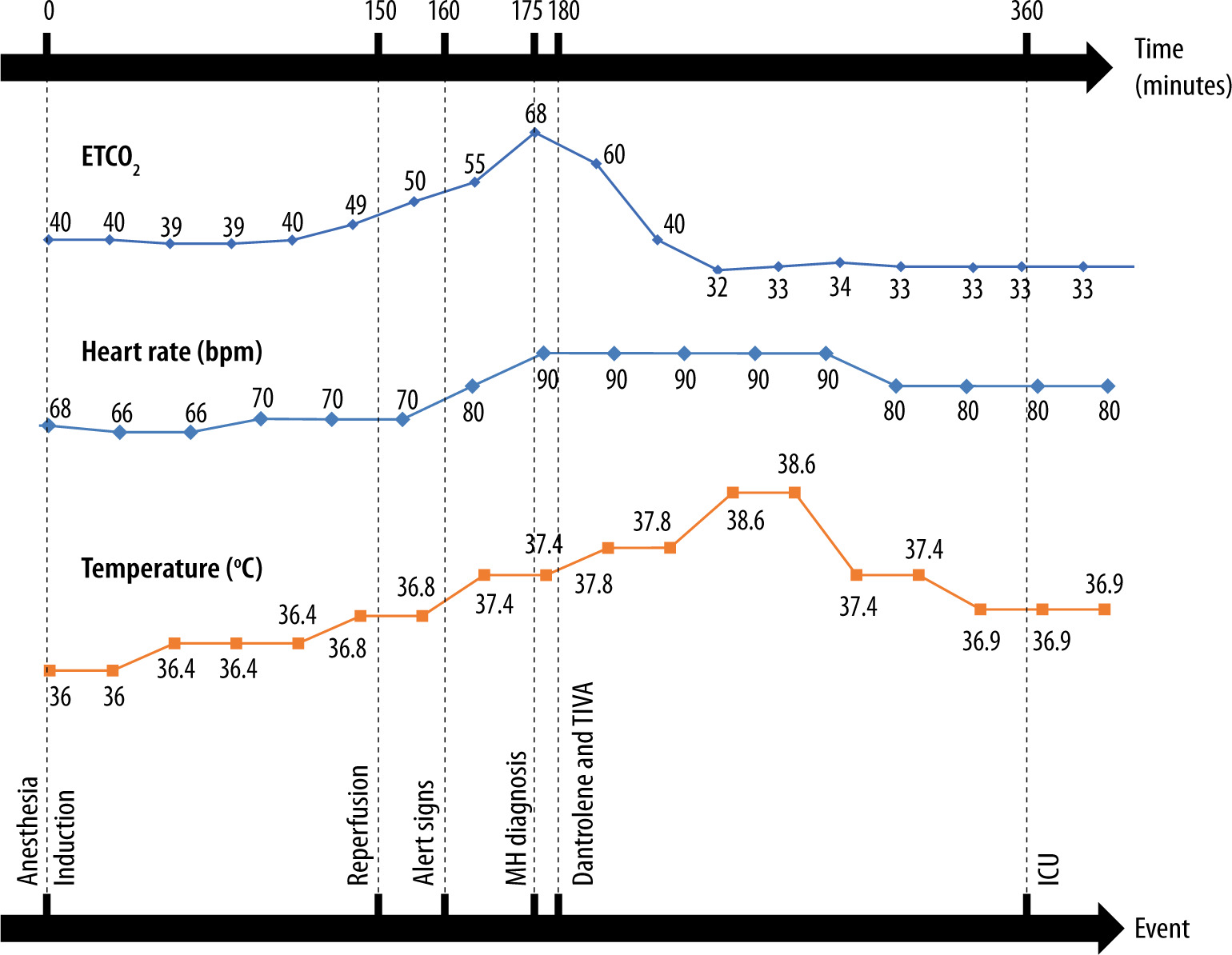
The patient was stable during the first 150 min, including during graft reperfusion. His ETCO2 ranged between 39 and 44 mmHg, SatO2 90–96%, HR 68–70 beats min–1, temperature 36–36.8oC, and BP 130–150 × 75-90 mmHg. Between 5 and 10 minutes after renal perfusion, his ETCO2 suddenly increased, reaching 68 mmHg, with no improvement despite an orotracheal tube change to discard internal obstruction and a volume-minute increase to 22 L min–1. Meanwhile, his temperature increased to 37.8oC, HR to 90 beats per min, and a surgeon informed the team about the rigidity of the patient’s abdominal wall. Arterial blood gas (ABG) analysis showed metabolic/respiratory acidosis and hyperkalemia (pH 6.92, PaCO2 79 mmHg, bicarbonate 16.2 mmol L–1, K+ 7.1 mmol L–1, BE –17). Fifteen minutes after the beginning of these changes, the clinical diagnosis of a suspected MH crisis was raised, the halogenated anesthetic was discontinued, total intravenous anesthesia (TIVA) was started, and dantrolene (2.5 mg kg–1) was administered in a single bolus. At this point, body cooling methods were not used to avoid hypothermia, because the temperature was under 38oC, and thereafter the patient presented only a transient increase of temperature until 38.6oC. Volume expansion was performed, and sodium bicarbonate and an insulin/glucose solution were administered. After dantrolene infusion, ETCO2 (32–35 mmHg) and temperature (36.9oC) normalized, abdominal muscle rigidity disappeared, and the patient’s volume minute returned to expected levels (6–7 L min–1). The new ABG analysis showed an improvement (pH 7.06, PaCO2 49 mmHg, bicarbonate 13.9 mmol L–1, K+ 7.6 mmol L–1, BE –15.9). Because of the maintenance of hyperkalemia, we administered more bicarbonate sodium and an insulin/glucose solution. The surgery was completed, and the patient was sent to the intensive care unit (ICU) sedated and under mechanical ventilation (Figure 1).
In the ICU, the patient was hemodynamically stable, and dantrolene (1 mg kg–1 every 6 h) was maintained for 24 h. On the first postoperative day, myoglobin peaked at 1.075 ng mL–1 and creatine phosphokinase (CPK) at 1.208 units L–1. On the second postoperative day, a new bolus of dantrolene was administered owing to an increase in ETCO2, followed by a further 24 h of dantrolene maintenance. The patient was extubated on the third postoperative day. Although the patient had no signs of DIC, he developed thrombosis of the renal vein and artery. The transplanted kidney was successfully removed on the sixth postoperative day with total intravenous anesthesia and decontamination of the anesthetic machine. The patient was discharged from the ICU on postoperative day 12 and from the hospital on postoperative day 23 without sequelae. After anesthesia, the patient informed us that his sister had a myopathy under investigation. The possibility of MH in the patient prompted the sister to undergo a molecular study, which showed a homozygous pathogenic variant in the ryanodine receptor gene (RYR1), pVal4844Ile. The patient refused muscle biopsy for the in vitro contracture test and did not undergo genetic testing.
We have described a suspected delayed-onset MH crisis in a male pa-- tient with end-stage CKD during kidney transplantation that was successfully managed but associated with transplant failure. The MH clinical grade scale [2] was 58, indicating an almost definite MH crisis (rank 6/6). This case report shows unusual aspects, such as its delayed-onset crisis, graft loss, an apparent good response to the first dose of dantrolene followed by recrudescence, and a family history of myopathy that was not observed during the pre-anesthetic evaluation. Although the patient refused muscle biopsy for the in vitro contracture test and did not undergo genetic testing, the presence of a homozygous pathogenic variant in the RYR1 gene in a first-degree relative suggests that the patient may be at least heterozygous for this variant and supports the diagnosis of malignant hyperthermia in this case.
Physiologic features of CKD patients, such as acidosis and hyperkalemia [5], may mimic MH presentation (Table 2). Besides those two characteristics, reperfusion syndrome may present with hemodynamic instability and hypercapnia [6, 16], which may also confound the MH crisis. Therefore, it is of utmost importance for anesthesiologists to discriminate the real cause when facing such alterations. Prompt diagnosis of MH and specific treatment define the morbimortality of the patient.
TABLE 2
Differential diagnosis of malignant hyperthermia, chronic kidney disease, and post-reperfusion syndrome
In our review of MH crisis during organ transplantation, the mean age of the nine patients was 32.67 ± 13.61 years (range 5–51 years), comparable to the age of our patient, and six of them were male (66.67%), consistent with the male predominance described in MH [1, 2]. The transplantation procedures were primarily those of the kidney, followed by liver and lung transplants. Eight patients received halogenated agents (one halo-thane, five isoflurane, two sevoflurane, and one not specified), and one received succinylcholine. The absence of triggering agents during anesthesia was reported in one case, but the anesthetic machine may have contained residues of halogenated agents, which could explain the crisis and the delay in its diagnosis. The mean interval of time between the beginning of anesthesia and the MH crisis was 2.81 ± 1.43 h, like the delayed-onset crisis of our patient. Desflurane is not as potent as isoflurane or sevoflurane [1], which could explain the delayed onset of the suspected MH crisis in our patient. Additionally, although he presented with elevated serum myoglobin and CPK levels, it was mild, like three of the nine previously reported cases. However, it is possible that metabolic problems related to CKD could have contributed to the delayed diagnosis in all cases.
The nine crises were described as typical cases of acute MH with a Clinical Grading Scale score between 5 and 6.
All nine reports used dantrolene as a specific treatment; there were no deaths described due to the MH crisis, and, unlike our case, none of them had graft loss or recrudescence after the crisis. A factor that could have contributed to the graft loss in our patient was thrombosis of the renal vessels. Thrombosis and hemorrhages associated with disseminated intravascular coagulation are complications of MH crisis [2] and were not reported in the other nine cases. However, during his hospital stay, the patient showed no changes in coagulation examination results.
Our patient experienced a suspected MH recrudescence, which occurs in nearly 25% of cases [2] despite the use of dantrolene, but it occurred later than usually described. In this case, we observed a delayed-onset crisis. This may be due to the low potency of desflurane. The high BMI (29.4 kg m–2) may also have contributed to the accumulation of desflurane in fat tissue and prolonged elimination time.
The possibility of RYR1-associated myopathy should always be considered when there is a family history of neuromuscular disorder, and this fact was unfortunately omitted by the patient. The anesthetist should actively inquire about this subject during pre-anesthetic evaluation.
In conclusion, MH diagnosis and treatment during organ transplantation are challenging, and anesthetists must be aware of possible differential diagnosis to minimize complications and transplant loss.