
Introduction
Venous thromboembolism (VTE), clinically manifested as deep vein thrombosis (DVT) or acute pulmonary embolism (PE), is the third most common acute cardiovascular syndrome following myocardial infarction and stroke [1]. The annual incidence of PE is between 39 and 115 per 100,000 inhabitants. The incidence of VTE is almost eight times higher in people aged 80 and older than in the fifth decade of life [2]. As a consequence, with the age of the population, long-term studies show an increasing tendency in the annual incidence rates of PE [3-6] over time. A recent analysis of relevant registration data from the World Health Organization (WHO) mortality database (2000-2015) found an average of 38,929 PE-related deaths each year in 41 countries of the WHO European Region (including Central Asia) representing a population of approximately 651 million [7]. Between 2000 and 2015, the annual age-standardized death rates associated with PE decreased by almost 50% (from 12.7 to 6.5 deaths per 100,000 inhabitants) with no significant gender differences. Despite this overall positive trend, the study also found that PE-related mortality continues to increase exponentially with age, reaching or even exceeding 80 deaths per 100,000 elderly population, and that PE also remains a relatively important cause of (in comparison with other causes) deaths among younger women, in which it accounted for up to 13 cases per 1000 deaths [8]. Since the outbreak of coronavirus disease 2019 (COVID-19), clinicians have struggled with the attempt to diagnose and manage the severe and fatal complications of COVID-19 appropriately. Several reports have described significant procoagulatory events, including life-threatening pulmonary embolism in these patients [9-51].
The incidence of PE in hospitalized COVID-19 patients is approximately 1.9-8.9% [36, 40, 50, 51]. The retrospective nature of the analyzed cohorts and relatively short observation periods could have underestimated the actual incidence of PE. Critically, COVID-19 patients requiring admission to the ICU seem to be at higher risk of thromboembolic complications, especially PE, which may occur in up to 26.6% of these patients [43]. In a prospective observational study involving 150 patients admitted to four ICU wards in two French hospitals, despite antithrombotic prophylaxis, the occurrence of PE was observed in 16.7% of treated patients [38]. The authors also reported that thromboembolic events occurred more frequently in patients with acute respiratory distress syndrome (ARDS) in COVID-19 patients compared to the historic ARDS cohort of a different etiology, underlining the unique procoagulatory effect of COVID-19 compared to other etiologies ARDS. In a retrospective cohort of 184 COVID-19 patients admitted to the ICU in three hospitals in the Netherlands, it was found that 13.6% of patients developed PE despite anticoagulation [39]. Interestingly, the incidence of PE increased to 33.3% when the follow-up period was extended from 1 to 2 weeks [46], at a time when increased awareness of the frequent occurrence of PE could lead to a higher rate of suspicion and extended diagnosis to detect this complication. Similarly, Poissy et al. found that 20.6% of patients admitted to the French ICU had pulmonary embolism on average 6 days after admission to the ICU despite the use of anticoagulants [41]. These authors also found that the incidence of PE in COVID-19 patients was twice as high as in patients admitted to the ICU as a control group and in 40 patients admitted to the ICU due to severe influenza.
Abnormalities in various coagulation parameters were frequently reported [49, 50] and were associated with poor prognosis [51]. It is common knowledge that all the time in cells there occur oxidation and reduction reactions which are connected with conversion of oxidation states of metals. Iron and nickel are able to generate free radicals through Fenton or Haber-Weiss reactions. These reactive oxygen species (ROS) are a potential danger to biological macromolecules and when defense mechanisms are insufficient, cytotoxic and genotoxic effects in cells can be observed. The study confirmed that iron can donate or accept an electron from neighboring molecules. This situation leads to damage of cellular components or to generation of reactive oxygen species. The Fenton and Haber-Weiss reactions, Fe2+ + H2O2 Fe3+ + HO. + OH- and Fe3+ + H2O2 Fe3 + HOO. + H+, describe the reactions of free iron with free radicals within a cell in order to generate more toxic radicals. These radicals can react with biomolecules such as DNA and cause them damage. Iron is involved in a number important metabolic processes including mitochondria transpiration, xenobiotic biotransformation, metabolism of lipids and proteins and DNA synthesis [52, 53]. Nickel can induce production of reactive oxygen species (ROS) and interact with nucleic acids, causing DNA damage. Unfortunately, little is known about the epidemiology and pathophysiological mechanisms underlying COVID-19-related PE due to the lack of extensive prospective studies in this context. Understanding these aspects is critical to the early diagnosis and appropriate management of this potentially fatal complication.
Material and methods
The retrospective study covered a group of 226 COVID-19 patients with division of the group of patients into groups with > 50% and < 50% lung tissue involvement, including patients with a radiologically confirmed pulmonary thrombotic event. The analyzed group consisted of 136 men and 90 women with mean age of 70 years. The groups were divided based on the percentage of the involved pulmonary tissue. Analyzed patients were hospitalized in the Provincial Specialist Hospital Cardinal Stefan Wyszyński in Lublin, 1st Military Hospital in Lublin, Agricultural Medicine Institute in Lublin.
All components were cataloged in accordance with the applicable regulations on sensitive data. Fe-dependent serum enzymes such as hemoglobin, ferritin, as well as zinc-related enzymes (C-reactive protein – CRP, D-Dimer) were analyzed. Each patient underwent high resolution computed tomography. The images were assessed by an experienced radiologist. The data collected in this way were compiled and analyzed using statistical tools. All statistical calculations were performed using the TIBCO Software Inc. statistical package. (2017). Statistica (data analysis software system), version 13. http://statistica.io. and an Excel spreadsheet. The study received full approval of the Medical University of Lublin Ethics Committee. Every single stage of the performed study was carried out in compliance with the Helsinki Declaration and national legislation.
Results
Two groups were distinguished among analyzed patients. The first group consisted of patients with < 50% of lung volume changes seen in the high resolution tomography scan, which covered 167 patients. The second group, with long volume changes over > 50, consisted of 79 patients.
Several different trace element dependent parameters were measured, a detailed descriptive analysis of which is presented in Tables 1 and 2.
Table 1
Presentation of gathered data in patients with < 50% of lung volume changes. N is the number of performed analyses of selected parameters. Some of the parameters were measured more than once
Table 2
Presentation of gathered data in patients with < 50% of lung volume changes. N is the number of performed analyses of selected parameters. Some of the parameters were measured more than once
Presented data were analyzed using the Spearman correlation coefficient, which revealed statistically significant results regarding analyzed parameters, which are presented in Table 3 (p < 0.05). In all of the presented parameters, a positive correlation was observed, except in the level of D-dimers. On the other hand, ferritin showed the strongest correlation among the presented parameters (Fig. 1).
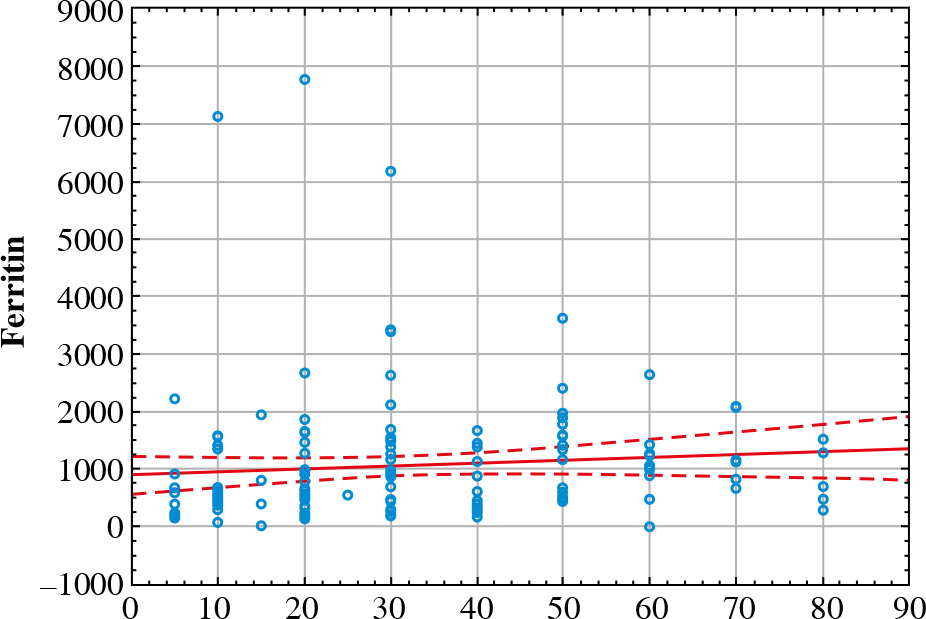
Table 3
Spearman correlation coefficient analysis results
| Variable | % lung volume changes |
|---|---|
| D-dimers | 0.077 |
| CRP | 0.230 |
| RBC | 0.138 |
| Hemoglobin (g/dl) | 0.166 |
| Hematocrit (%) | 0.169 |
| Ferritin | 0.271 |
In the next step the analysis of both groups was performed, using the Mann-Whitney U-test, which showed statistically significant results between groups. The group consisting of patients with < 50% of lung volume changes had higher parameter values in each analyzed parameter, except RBC (p < 0.05). Especially, the level of ferritin was much higher in the first group (p = 0.000008). Elevated ferritin levels were observed in all patients with COVID-19 involvement of lung tissue.
Discussion
Iron plays a very important role due to its biological activity by regulating enzymatic activity and oxidation and reduction reactions [52]. Iron is involved in a number important metabolic processes including mitochondria transpiration, xenobiotic biotransformation, metabolism of lipids and proteins and DNA synthesis [53]. Iron crosses membranes as the ferrous form (Fe2+) and in this process a few enzymes and a divalent metal transporter are involved. This metal is carried by transferrin in ferric form but in the cell it is stored within ferritin. The ferric ions need reduction to the ferrous form through the Fenton reaction and then they can be released in cells. This process is connected with generation of ROS which cause oxidative stress in cells such as damaged cellular membranes and nuclei. Free forms of iron are toxic and detrimental for cells but binding by molecules is involved in that [54]. This metal is linked in plasma by transferrin, which has two iron-binding sites. In addition, iron in the cytosol is stored inside the ferritin which, when necessary, can release metal ions.
Ferritin was previously described as an acute phase factor as well as an indicator of dysregulation of the immune system in COVID-19 patients. Moreover, its role was underlined in the cytokine storm process. Ferritin was found to moderate the expression not only of the pro-inflammatory but also the anti-inflammatory cytokines. Moreover, Marcinkiewicz et al. suggested that interleukin (IL)-6, along with other cytokines, drives an acute phase response that elevates serum ferritin [55]. In the study performed by Carubbi et al. higher ferritin levels as well as D-dimer levels were linked to severity of pulmonary involvement but not associated with the outcome [56]. They speculated on the role of ferritin in pathogenesis of lung damage but underlined the need for further research supplemented with radiological analysis. Moreover, different studies reported higher ferritin levels in patients with pulmonary embolism caused by COVID-19 compared to non-pulmonary embolism patients [57, 58]. In this study patients with severe COVID-19 complicated with pulmonary embolism were analyzed. Based on the lung volume involved, assessed in the HR CT scan, two groups were distinguished. Interestingly, contrary to the previously mentioned study, the first group with lung volume involvement < 50% turned out to have higher ferritin (p = 0.000008) and D-dimer (p = 0.036) levels compared to the second group (Table 4).
Table 4
Comparison of results in both analyzed groups
In the study performed by Mulder et al. no associations were observed for higher D-dimer, higher CRP or higher ferritin concentration and clinical pulmonary thromboembolism. However, they observed a lower ferritin concentration, in patients with, compared to those without, clinical pulmonary thromboembolism [59]. Contrary to those results, in this study elevated levels of each parameter were observed; however, those parameter were higher in the second group.
Conclusions
The study demonstrated that elevated levels of several inflammatory and thrombotic parameters such as ferritin, D-dimer, CRP as well as hemoglobin do not correlate with the degree of lung tissue involvement in the computed tomography image. The study compared patients with a known thrombotic pulmonary event. The study did not compare the ferritin levels in patients with pulmonary tissue involvement in the group with and without known pulmonary embolism. This area of research should be deepened in view of the role of ferritin as a predictor of pulmonary embolism.