









Introduction
Cardiovascular disease prevention is pivotal in decreasing the number of hospitalizations and deaths attributable to cardiovascular disease, especially in patients at elevated risk for cardiovascular disease, such as metabolic dysfunction-associated steatotic liver disease (MASLD) patients [1]. MASLD represents one of the most common chronic liver conditions worldwide, with prevalence rates paralleling the rising trends of obesity and metabolic syndrome [2]. The multifactorial pathophysiology of MAFLD underscores the significance of preventive and therapeutic strategies that tackle multiple aspects of the disease. Accumulating evidence indicates the potential of lifestyle modification, especially dietary alterations, in the management and even reversal of liver steatosis [3]. A balanced lifestyle is said to impact the individual’s health substantially. It has been emphasized that neither genes nor health care significantly impacts individuals’ health more than the appropriate lifestyle [4].
Dietary habits are a significant component of a healthy lifestyle and closely correlate with religious beliefs [5]. An important period in the Catholic calendar is the 40 days of Lent associated with fasting. The type of fast during Lent is not strictly defined and depends on an individual’s beliefs. Some limit themselves to fasting only on Good Friday, while others fast for the entire 40-day period. There are differences also in the approach to the types of meals – from avoiding alcohol, meat, sweets, snacks, or sweetened drinks to limiting eating to once per day.
Aim
Fasting changes the diet and potentially has an impact on cardiovascular risk. The study aimed to evaluate if the declared type of fasting during Lent influences cardiovascular health in terms of the most common cardiovascular risk factors control in patients with MASLD.
Material and methods
The study was designed as a prospective, observational cohort study. It consisted of 210 MASLD participants and was conducted during Lent. All patients were screened for cardiovascular risk factors and were post factum diagnosed with MASLD according to the current criteria [6]. MASLD diagnosis required evidence of hepatic steatosis by imaging or histology with at least one out of 5 criteria:
body mass index (BMI) ≥ 25 kg/m2 (23 in Asians) or waist circumference > 94 cm (in males) or 80 cm (in females) or ethnicity adjusted,
fasting serum glucose ≥ 5.6 mmol/l (100 mg/dl) or 2-hour post-load glucose levels ≥ 7.8 mmol/l (≥ 140 mg/dl) or glycated haemoglobin (HbA1c) ≥ 5.7% (39 mmol/l) or type 2 diabetes or treatment for type 2 diabetes,
blood pressure ≥ 130/85 mm Hg or specific antihypertensive drug treatment,
plasma triglycerides ≥ 1.70 mmol/l (150 mg/dl) or lipid-lowering treatment,
plasma HDL-cholesterol ≤ 1.0 mmol/l (40 mg/dl) in males and ≤ 1.3 mmol/l (50 mg/dl) in females or lipid-lowering treatment.
The diagnosis was made only when other causes of steatosis (including excessive alcohol intake) were excluded.
In the beginning, all participants were asked about a history of smoking and a physical examination was conducted to evaluate weight, height, BMI, systolic blood pressure (SBP), diastolic blood pressure (DBP), and heart rate (HR). In the next step, a sample of blood was collected from each participant to assess basic parameters, including total cholesterol level (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein (LDL-C), triglycerides (TG), HbA1c, and estimated glomerular filtration rate (eGFR) calculated by MDRD formula. Then individuals were divided into 2 groups. Participants from the first group (group A) were self-declared Catholics willing to fast strictly for the whole Lent period, which meant avoiding consuming alcohol, meat, sweets, snacks, sweetened drinks, etc. In the second group (group B), participants were fasting the same way only on Good Friday while maintaining regular dietary habits on all the other days. After 40 days of observation, all participants were examined and had blood taken for the same assessment as during enrolment. Both groups were then compared in terms of cardiometabolic health measures.
Statistical analysis
All statistical analyses were performed using SPSS (SPSS version 26, Inc., Chicago, IL) for macOS. Obtained data were tested for normality using the Kolmogorov-Smirnov test. Data showing continuous distribution are presented as mean and 95% confidence intervals (CI), and their comparisons were made using the Mann-Whitney test or Student’s t-test. The categorical variables were compared using the χ2 or Fisher exact tests. A p-value of less than 0.05 was considered statistically significant.
Results
The study consisted of 210 participants with a mean age of 56.0 ±6.6 years. 148 (70.5%) were male. None of the included patients had a history of cardiovascular disease, including no cases of previously diagnosed arterial hypertension. Detailed characteristics of the study population are presented in Table I.
Table I
Baseline characteristics of the study population
The population was divided according to the chosen type of fasting. Group A (strict fasting) consisted of 104 participants. Most of them were men (66.3%). The mean age was 56.1 ±6.8 years. As for the cardiovascular risk factors, almost half of the patients were obese (48%), and about one-third were smokers (36%). Group B included 106 Catholics, who were predominantly male (74%). Those patients were at a similar age as group A (55.8 ±6.4 vs. 56.1 ±6.8 years) but had a lower prevalence of obesity (41% vs. 48%) and smoking (25% vs. 36%).
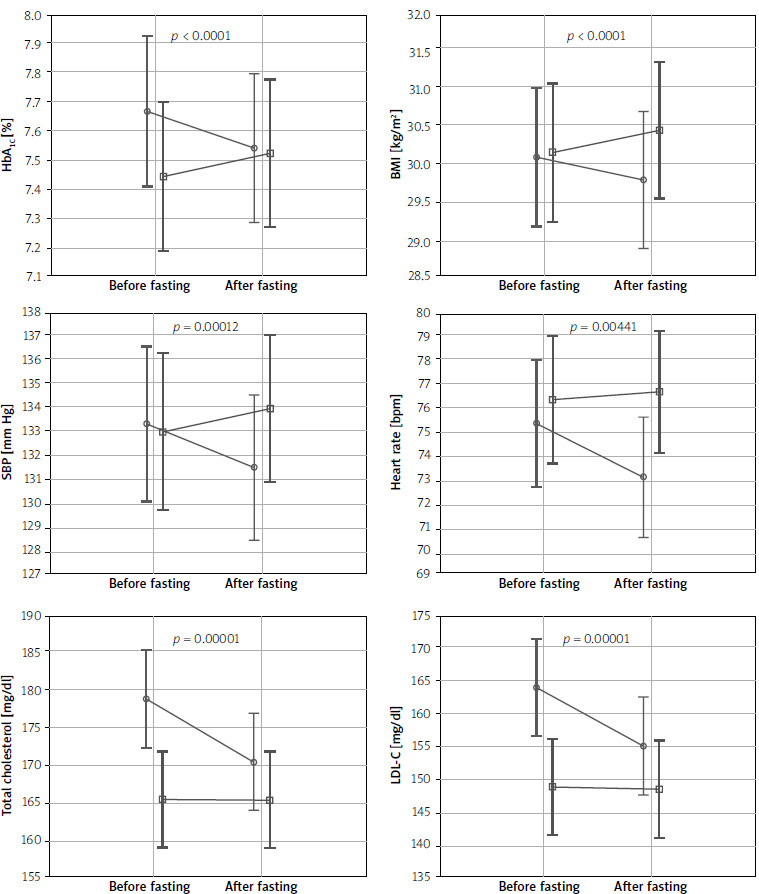
After 40 days of fasting, in group A a beneficial decrease in almost all parameters was observed, whereas in group B no differences were noted. Moreover, in group B there was an inconsiderable increase in the HbA1c levels (7.44% vs. 7.52%) and blood pressure values (132.97 mm Hg vs. 133.9 mm Hg for SBP and 81.28 mm Hg vs. 81.3 mm Hg for DBP).
Comparison of both groups before intervention indicated statistically significant differences in the lipid profile, with particular importance in terms of total cholesterol levels (178.71 mg/dl vs. 165.55 mg/dl, p = 0.004) and LDL-C (163.87 mg/dl vs. 148.9 mg/dl, p = 0.004). Differences in the most important cardiometabolic health measures before and after fasting are presented in Table II and Figure 1.
Table II
Comparison of main parameters between groups
Discussion
Cardiovascular disease is the most common cause of mortality and morbidity worldwide. Despite significant improvements in pharmacotherapy and treatment methods, they remain a severe challenge in everyday clinical practice. According to the Global Burden of Disease Study, cardiovascular diseases are responsible for more than 15 million deaths in 2010 and 4 million in Europe [7]. This constant high rate prompts the search for ways to reduce mortality and morbidity, especially in high-risk populations such as MASLD patients, one of which might be an improvement of dietary habits.
MASLD is a new term that recently replaced and modified diagnostic criteria for long-used nonalcoholic fatty liver disease (NAFLD) [6]. Most current studies assessing the impact of liver steatosis on cardiovascular risk include NAFLD patients. Nevertheless, it was shown that hepatic steatosis is a risk factor for atherosclerotic cardiovascular disease morbidity and mortality [8].
Faith has an undoubted influence on health. Studies show that religious participation is associated with lower levels of many cardiovascular risk factors, including waist-to-hip ratio, TC, SBP, DBP, and C-reactive protein. However, such a correlation was not observed in the context of BMI and HbA1c [9, 10]. According to the current guidelines, a well-balanced diet is the basis of lipid-lowering treatment [11]. Religious beliefs have a considerable influence on our habits, including diet. In the Japanese retrospective study, based on data collected between 2005 and 2010 among individuals who underwent annual health check-ups, it was proven that patients who declared as religious paid more attention to healthy habits, resulting in fewer cardiovascular risks [12]. The same conclusions may be drawn from the Greek study conducted on a group of 1519 rural citizens of Greece. After 12 years, it was observed that participants who declared themselves to be moderately religious were found to have decreased risk for all-cause mortality, including cardiovascular death [13].
Studies show that intensive control of cardiovascular risk factors, including achieving very low LDL cholesterol levels, contributes to a persistent reduction of cardiovascular events [14]. Nevertheless, sole lifestyle modification is often inefficient, and patients still require pharmacotherapy. While fasting is only one of the potential additions to complex treatment and lifestyle modifications, it may contribute to the reduction of not only cardiovascular risk but also the risk of diseases such as metabolic dysfunction-associated steatotic liver disease [15].
Among numerous religious practices, fasting is particularly relevant. Several religious groups spend a certain period each year fasting. Its spiritual role is usually attributable to spiritual purification. In different religions, fasting is limited to caloric restriction, with or without excluding certain types of food, but it may also focus on avoiding all food intake during specific periods. Most of the available analyses of the influence of fasting on health focus on Islamic Ramadan, the Greek Catholic Nativity Fast, or Daniel Fast. A large meta-analysis from 2019 confirmed a significant reduction in fat tissue between the pre-Ramadan and post-Ramadan periods, especially in overweight and obese individuals [16]. A Bible-based Daniel Fast involves a 21-day ad libitum food intake period, devoid of animal products and preservatives and inclusive of fruit, vegetables, whole grains, legumes, nuts, and seeds. One of the studies showed that Daniel Fast is associated with improved cardiovascular parameters, including total cholesterol, LDL-C, HDL-C, SBP, and DBP [17].
Faith has also been proven essential in improving recovery after cardiovascular incidents, including myocardial infarction. For example, an analysis of 2067 American patients hospitalized due to acute coronary syndrome between 2011 and 2013 revealed that those strongly involved in religious practices were more involved in the convalescence process and thus had better prognoses [18].
Our study showed that in the group of people with MASLD, a more significant number had slightly elevated lipid levels at baseline, in most cases without realizing it. Other measures of increased cardiovascular risk were also present. Moreover, in our study, stricter fasting was strongly associated with better control of cardiovascular risk factors after Lent. Group A, where dietary restrictions were stricter, achieved better results in almost all examined parameters. The relatively short period of diet improvement translated to a possible improvement in prognosis.
It has been shown that even a slight decrease in parameters such as SBP or LDL-C is responsible for decreasing the risk of cardiovascular events and mortality [19, 20]. Moreover, clinical nutritional societies debate whether orthodox religious fasting should be considered a form of dyslipidaemia treatment [21]. Nevertheless, it is worth emphasizing that our observation concerned only the 40-day Lent period, and it is necessary to consider another long-term study in the future.
Conclusions
The study showed that in patients with metabolic dysfunction-associated steatotic liver disease, strict dietary restrictions are associated with a significant improvement in risk factors and measures of cardiometabolic such as LDL-C, HbA1c, and blood glucose. In these settings, short-term lifestyle modification is the first step in improving the general prognosis and reducing the cardiovascular risk burden. Nevertheless, lifestyle changes must cover many areas of life and, in many cases, will not replace appropriate pharmacotherapy.