







Introduction
The incidence of gastric cancer in the upper portion of the stomach is continually increasing in Eastern and Western countries [1, 2]. Because early gastric cancer has an excellent long-term prognosis and the 5-year survival rate is higher than 90%, quality of life after a gastrectomy is very important for patients [3, 4]. Preserving a larger part of the stomach contributes to improving the postoperative nutritional status, maintaining body weight, and improving postoperative quality of life [5]. Therefore, proximal gastrectomy (PG) has been suggested as an alternative to total gastrectomy (TG) [5, 6]. Several studies have proved that PG has advantages over TG – it is associated with a shorter operation time, earlier recovery, and better postoperative nutritional status [7–9]. The Japanese gastric cancer treatment guidelines recommend PG as an alternative procedure for early gastric cancer located in the upper portion of the stomach [10]. However, Kunisaki et al. reported that only a small proportion of institutes (21.8%) perform PG for patients with early gastric cancer located in the upper third of the stomach [11].
Accordingly, three types of reconstruction after PG have been introduced: esophagogastrostomy (EG stomy), jejunal interposition (JI), and double tract reconstruction (DTR). Although PG with EG stomy is a simple and feasible method, it is associated with a high risk of postoperative complications such as reflux esophagitis, which causes severe heartburn, chest pain, and regurgitation of sourness, stenosis, and residual food [5, 7, 12–19]. Hence many surgeons abandoned this reconstruction, and adopted tube-like stomach EG stomy [13, 16, 20–22]. They found that tube-like EG stomy had a lower incidence of stenosis and reflux esophagitis than traditional EG stomy. Recently, laparoscopic JI and DTR have been widely adopted for laparoscopic PG because many surgeons overcame several technical difficulties of totally laparoscopic total gastrectomy (TLTG).
Some studies have shown that LPG with DTR (PG-DT) could be used to avoid anastomotic complications [23, 24]. In one study, the incidence of reflux symptoms, usage of proton pump inhibitors, and anastomotic strictures were significantly lower in the DTR than in the EG stomy group [23]. Li et al. performed a meta-analysis to compare the use of LPG-DTR and TG for proximal early gastric cancer [25]. They concluded that PG-DTR is comparable to TG for patients with proximal early gastric cancer, and reported that LPG-DT not only appears superior to TG in terms of preventing vitamin B12 deficiency, but also does not increase the risks of anastomotic stricture and reflux esophagitis. However, a recent multicenter study conducted in Italy showed that PG is associated with a higher mortality rate and higher risks of reflux esophagitis and anastomotic stricture than TG [26].
Aim
This study was performed to investigate the feasibility, safety, and incidence of postoperative complications including reflux esophagitis and stricture of LPG with DRT.
Material and methods
We retrospectively collected and analyzed data on 37 patients who underwent curative LPG with DTR as treatment for upper third gastric cancer between December 2013 and December 2018. All patients underwent totally laparoscopic PG with intracorporeal DTR. We evaluated TNM stage using the classification guidelines presented in the eighth edition of the American Joint Committee on Cancer Staging Manual. Numerous clinico-pathologic data were evaluated. Also, we evaluated postoperative complications (Clavien-Dindo classification), safety, effectiveness and feasibility. Additionally, the postoperative nutritional status and short-term oncologic outcomes of the patients were evaluated. This study was approved by the institutional review board (2019-0702).
Surgical procedures
Less than half of the proximal stomach was laparoscopically resected. We performed side-to-side intracorporeal esophagojejunostomy (EJ stomy) via the overlap method using a 45 mm linear stapler (Photo 1 A). Following this, we closed the common hole transversely to prevent narrowing of the anastomosis between the esophagus and jejunum using 60 mm linear staplers and three stitches. Photo 1 B shows the final view after EJ stomy. We then performed gastrojejunostomy (GJ stomy) about 10–15 cm away from the EJ stomy site using two 60 mm linear staplers (Photos 1 C and D). Lastly, intracorporeal jejunojejunostomy was performed about 20 cm away from the GJ stomy site using two 60 mm linear staplers (Photos 2 A and B). Photo 2 C shows the final view after LPG with DTR. Photo 3 shows the endoscopic findings 6 months after LPG and DTR.
Photo 1
A – Intracorporeal esophagojejunostomy using 45 mm linear stapler, B – final anastomosis view after esophagojejunostomy, C – intracorporeal gastrojejunostomy using 60 mm linear staplers, D – final anastomosis view after gastrojejunostomy
E – esophagus, J – jejunum, ST – stomach.



Results
Basic clinicopathologic characteristics
The clinicopathologic characteristics of all patients are summarized in Table I. A total of 37 patients were included in this study, 25 (70%) of whom were male and 12 (30%) of whom were female. The mean age of the patients was 61.2 ±9.5 years. Overall, 31 (83.7%) patients were diagnosed with gastric cancer, 5 (13.5%) with gastrointestinal stromal tumors (GISTs) and 1 (2.8%) with leiomyoma. Moreover, 19 (51.3%) had comorbidities and 4 (10.8%) had undergone prior abdominal surgery. Two patients underwent cholecystectomy or hiatal hernia repair at the same time as LPG-DTR. There was no conversion to open surgery during the operation. All patients underwent LPG with DTR and all procedures were performed intracorporeally.
Table I
Clinicopathologic characteristics of all patients (n = 37)
Clinicopathologic outcomes of patients with gastric cancer
The outcomes of the patients with gastric cancer are summarized in Table II. The mean operative tine was 171.4 ±29.4 min. The mean length of hospital stay after surgery was 7.45 ±1.84 days and the mean time to first flatus after surgery was 3.43 ±0.94 days. Overall, 27 patients had stage IA gastric cancer and none had > stage 2A. We evaluated complications using the Clavien-Dindo classification; there were 3 (9.6%) complications. However, there was no complication of grade 3 or above. We did not observe any postoperative mortality or recurrence after surgery.
Table II
Clinicopathologic outcomes of patients with gastric cancer (n = 31)
Endoscopic surveillance
One patient with a GIST did not undergo endoscopic surveillance. Moreover, 3 patients were not evaluated for the distal stomach because the endoscopist incorrectly thought that they had undergone TG. The remaining 33 patients underwent complete postoperative endoscopic surveillance. Table III shows the pre- and postoperative endoscopic findings. A total of 63.6 patients had gastritis or atrophic gastritis before surgery, but only 13 (39.4%) exhibited gastritis/atrophic gastritis during the postoperative endoscopic examination. Moreover, 3 (9%) patients were diagnosed with reflux esophagitis during the preoperative endoscopic examination, but none exhibited reflux esophagitis after surgery. In addition, none of the 33 patients developed postoperative reflux esophagitis. Moreover, we did not observe stenosis or stricture at the EJ stomy or GJ stomy site. One patient was diagnosed with a gastric ulcer and another with a duodenal ulcer. Both were successfully treated with medication.
Nutritional outcomes and body weight changes
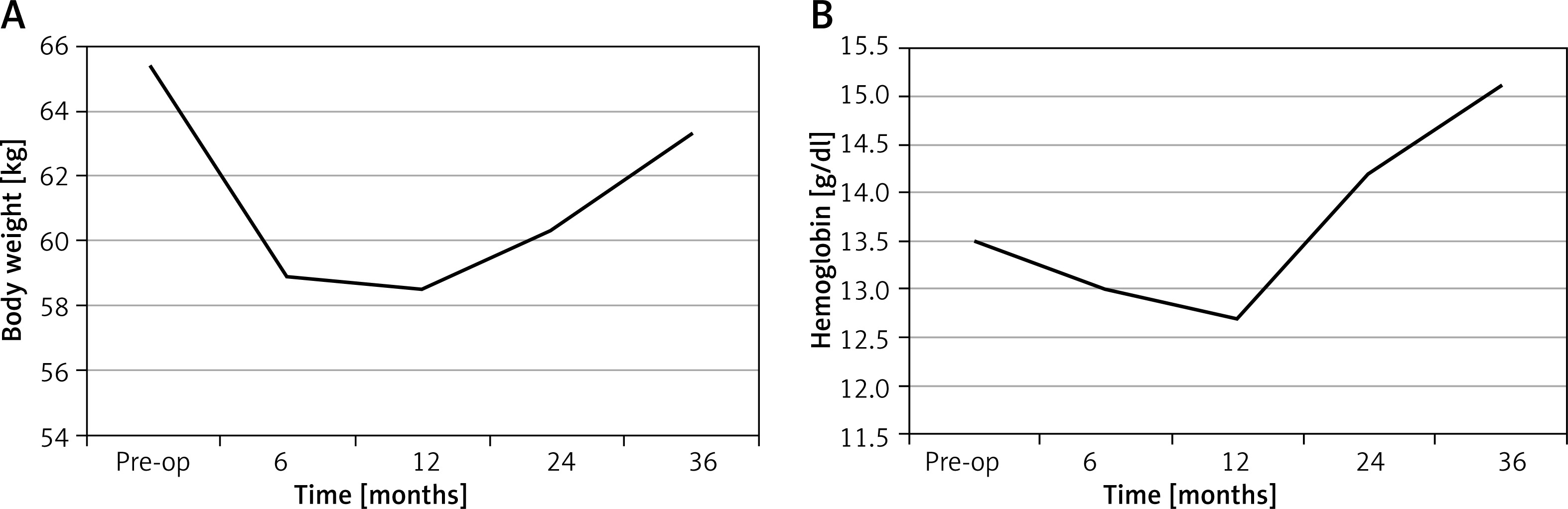
The postoperative nutritional outcomes and body weight changes of the patients are summarized in Table IV and Figures 1 and 2. Maximum weight loss was observed 1 year after surgery (6.9 kg, 10.5%). Following this, the body weight of the patients gradually increased and recovered to 96.8% of their preoperative body weight 3 years after surgery. Likewise, serum hemoglobin level decreased maximally (0.8 g/dl, 5.9%) 1 year after surgery and increased thereafter, and it was higher than preoperative hemoglobin level from 2 years after surgery. The iron levels of the patients increased after surgery and were highest 2 years after surgery. However, the vitamin B12 levels of the patients were lowest 6 months after surgery and fluctuated thereafter. In contrast, albumin level was higher than the preoperative level from 6 months after surgery.
Table IV
Nutritional outcomes and body weight changes after surgery

Discussion
PG has gradually replaced TG as the surgical method of choice for gastric cancer in the upper third of the stomach because PG has similar oncological outcomes to TG and the reservoir capacity of the stomach [27–29]. It is well established that early gastric cancer located in the upper third of the stomach is rarely associated with lymph node metastasis at number four d, fiver and six [10, 30, 31]. Thus, the Japanese Gastric Cancer Association and Korean Gastric Cancer Association recommend that PG be used to treat early gastric cancer located in the upper third of the stomach [10, 32].
Laparoscopic total gastrectomy (LTG) was first reported in 1999 [33]. It is practiced less widely and is more challenging to perform because the procedure is associated with a high risk of bleeding and a technically demanding anastomosis, all within a narrow operating field [34–36]. However, as a result of technical advances and improved instrumentation, various techniques of intracorporeal EJ stomy have been introduced. Thus, TLTG was widely accepted for gastric cancer in the upper third of the stomach and the use of LPG has gradually increased. Recently, a number of studies comparing TLTG and conventional open TG for gastric cancer located in the upper third of the stomach have shown it to be feasible, effective, and safe [22, 37, 38]. In this study, we performed all PG using totally laparoscopic surgery with intracorporeal anastomosis without postoperative mortality or severe complications.
We did not investigate PG with EJ stomy because a number of studies showed that PG with EG stomy was associated with a higher incidence of complications such as reflux, stenosis, and stricture than TG [15, 23, 39]. Furthermore, several studies reported that there was no significant difference in surgical outcomes between LPG with DTR and LTG [3, 24, 25, 27, 40–42]. In a previous study, LPG with DTR did not increase the incidences of reflux esophagitis and anastomotic stenosis compared to LTG. Moreover, the incidence rates of reflux esophagitis and anastomotic stenosis were lower in the PG with DTR group than in the PG with EJ stomy group [11]. Thus, we concluded that LPG with DTR is a feasible and safe treatment option for early gastric cancer located in the upper third of the stomach.
Quality of life including nutritional issues is an important problem especially for patients with early gastric cancer or benign disease. Many studies have reported that LPG had nutritional benefits and a good quality of life. Kim et al. reported that patients who underwent LPG with DTR had higher iron and vitamin B12 absorption rates than those who underwent LTG [41]. Jung et al. showed that the body weight change in LPG with DTR is lower and the vitamin B12 level is higher than the LTG group [27]. Sugiyama et al. observed that the body weight and skeletal muscle index reduction rates were lower in the LPG-DT group than in the LTG group [42]. Recently, Tanioka et al. reviewed 11 articles (336 underwent LPG and 547 underwent LTG) to evaluate surgical outcome and nutritional outcomes [43]. The LTG group had a significantly lower body weight and LPG had a weighted mean difference. Also, total protein, albumin and the total lymphocyte count were less likely to decrease in the LPG group.
The present study has some limitations. First, this was a retrospective study performed at a single institute. Second, the number of enrolled patients was relatively small. Third, we did not evaluate long-term oncologic outcomes. Lastly, this was a single arm study.