









Von Meyenburg complexes, also known as biliary hamartomas, are rare benign malformations of the intrahepatic bile ducts, caused by the failure of embryonic bile duct involution [1]. It is usually asymptomatic, so it usually represents an incidental finding in liver imaging [2]. Despite being benign lesions, von Meyenburg complexes can create clinical challenges, such as differentiation with other more relevant pathological conditions [3]. Therefore, liver imaging with magnetic resonance imaging (MRI) or magnetic resonance cholangiopancreatography (MRCP) is recommended [4, 5].
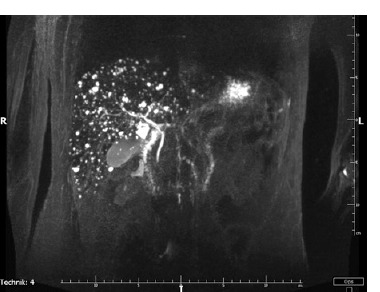
A 34-year-old man was referred to a gastroenterology outpatient clinic due to periodically recurring severe abdominal pain and non-bloody diarrhoea for several years. The patient had not been treated chronically. An important part of his medical history was an appendectomy complicated with an abscess in the postoperative wound area a year earlier. No abnormalities were found in laboratory and endoscopic examinations. Due to the clinical suspicion of Crohn’s disease, MR enterography was performed, which showed inflammatory changes of low activity in the ileocaecal area. In addition, dilatation of the peripheral segments of the intrahepatic bile ducts was found. Subsequently, MRCP was performed, which showed multiple minor hyperintense lesions described as “starry sky”, which corresponds to von Meyenburg complexes - a developmental malformation of the intrahepatic bile ducts of the hamartoma type (Figure 1). In addition, the intrahepatic and extrahepatic bile ducts were normal. Considering the clinical characteristics and typical MRCP images, the diagnosis of von Meyenburg complexes was made.
Figure 1
Magnetic resonance cholangiopancreatography: multiple small lesions evenly dispersed in both liver lobes, with a “starry sky” appearance
Von Meyenburg complexes are rare benign liver malformations characterised by cystic dilated biliary ducts [6]. These cystic hepatic lesions do not communicate with biliary tracts and can range in size from up to 1.5 cm. They are similar to each other and countless, giving the appearance of a “starry sky” [7]. The estimated prevalence of von Meyenburg complexes is around 1% in imaging techniques [6]. In the differential diagnosis liver metastases, intrahepatic stones, peribiliary cysts, and Caroli’s disease should be considered [3, 5]. It is generally asymptomatic; however, several case reports have suggested the possible malignant transformation of biliary hamartomas into cholangiocarcinoma and hepatocellular carcinoma [8]. To date, the occurrence of von Meyenburg complexes concomitant with Crohn’s disease has not been described [9]. A proper diagnosis is established when typical imaging findings are present; otherwise, histological confirmation might be required [10]. No specific treatment is necessary for these lesions [6]. Currently, there are no standard guidelines for the diagnosis and treatment of biliary hamartomas. More research is needed to determine the best surveillance strategy for these patients also in the context of the course of inflammatory bowel diseases.