







Introduction
Injections of botulinum toxin A (BTX-A) administered to the bladder wall have been a well-established method in the treatment of refractory idiopathic overactive bladder (RIOAB) for many years now. According to the definition proposed by Phe et al. [1], RIOAB is recognized in the absence of the effects of pharmacological treatment or its discontinuation due to adverse effects. In order to achieve the therapeutic effect of BTX-A in RIOAB therapy, it is important to properly deposit the drug within the bladder wall. There are two options described in the literature; the first one consists of injections into the detrusor muscle, which remains the standard treatment technique approved by the US Food and Drug Administration [2, 3]. The second method consists of submucosal injections, which reportedly are equally effective and may allow for more precise distribution of the drug [4]. Nevertheless, both methods require great meticulousness: if the insertion is too shallow, it may cause extravasation of the drug into the bladder cavity, whereas if it is too deep, the administration of the drug may go outside the bladder, sometimes intraperitoneally. Although there are no data on the possible side-effects of such a situation, it obviously means a partial loss of the dose of the drug, which may affect the final therapeutic effect.
Routinely, BTX-A should be administered evenly over the entire surface of the bladder, omitting the bladder trigone, in order to avoid the risk of vesico-ureteral reflux – even though previous studies have not confirmed the occurrence of this phenomenon. However, the current guidelines continue to recommend excluding the bladder trigone [5, 6].
According to the standard protocol, the drug solution is prepared with 0.9% NaCl. The resulting mixture is colorless, which renders any observation of the spilled volume of the drug impossible. Moreover, puncture sites are often poorly visible as well, which becomes an even greater issue in case of bladder bleeding. In such situations, achieving even distribution of injections can be difficult. A potential solution to this problem may be the addition of a dye to the BTX-A solution. This study presents and discusses the results of treatment of patients with RIOAB using botulinum toxin with the addition of methylene blue (MB).
Aim
Evaluation of the results of RIOAB treatment with BTX-A with the addition of MB in comparison to the standard method.
Material and methods
This clinical trial was designed as a prospective, single-blind (patient-blind), randomized trial.
We screened, blinded, and randomly selected our subjects from a group of eighty patients with RIOAB diagnosed through a urodynamic study and 2-day bladder diary. Patients had been inadequately managed by anticholinergic or B-mimetic therapy (insufficient efficacy during at least 3 months of treatment or intolerable side effects). Enrolled patients experienced at least 3 urinary urgency episodes in a 2-day bladder diary, an average of ≥ 8 micturitions per day, and a postvoid residual (PVR) urine volume ≤ 100 ml. Patients had to be willing to initiate clean intermittent catheterization (CIC) after treatment, if necessary. The patients were divided into two groups: a BTX-A with MB group, and a non-MB control group.
The following exclusion criteria were applied: previous lower urinary tract surgery, active urinary tract infection (UTI), impaired renal function, neurologic disease, bladder disease affecting bladder function, severe coagulopathy, bladder outlet obstructs (BOOs), active hematuria, deficiency of glucose-6-phosphate dehydrogenase, diabetes, pregnancy, inability to complete the questionnaire form.
Flow diagram
Eventually, seventy-five randomly selected patients were analyzed in the study. The average age was 45.6 (range: 19–81). The study was conducted between February 2014 and December 2017. The severity of RIOAB, including frequency, nocturia, urgency and episodes of urinary incontinence, were assessed using the Overactive Bladder Symptom Score (OABSS). Global changes in the quality of life were assessed using the Likert scale. In each case a dose of 100 IU of botulinum toxin A (Botox) was used. For the group treated with MB the drug was dissolved in 9.5 ml of 0.9% NaCl. In each case 0.5 ml of MB 1% (10 mg/ml) was added to the solution of the drug, which resulted in its coloring. The study was approved by the local research ethics committee. All the patients provided their written informed consent before participation. The safety of using the BTX-A solution with the addition of MB has been pharmacologically tested; we have presented the results of these studies in our previous publication (Figure 1) [7].

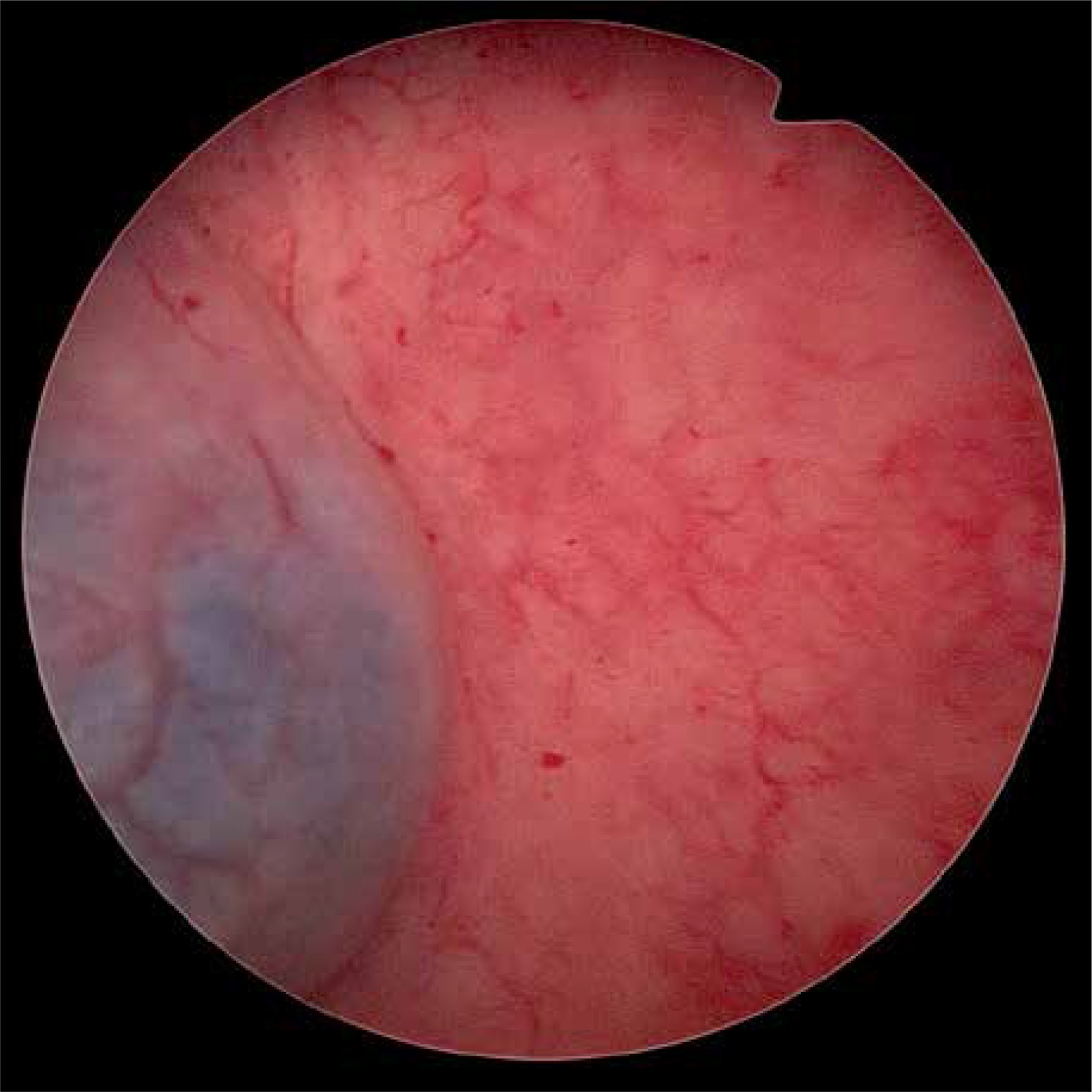
Following our primary observations, a fixed dose of 0.5 ml of methylene blue proved to be the smallest dose which effectively improved the intraoperative observation. For the group without MB the drug was dissolved in 10 ml of 0.9% NaCl. The injections were performed submucosally during cystoscopy using a 3.7 Fr Williams cystoscopic injection needle (Cook Urological, Specer, IN, USA) into 20 injection sites. The procedure was performed using short intravenous anesthesia. In each case the bladder was filled with 200 ml of saline. After the procedure, a Foley catheter was placed and then removed when the patient was discharged. Installing the catheter provided good drainage of urine in the postoperative period and enabled us to monitor the amount of bleeding. In the case of urinary retention or increase of the PVR over 200 ml, the patient was instructed to have a CIC (Photos 1, 2).

Urinalysis and urine culture were performed fourteen days after treatment and in this clinic visit PVR was re-evaluated by ultrasound examination. If PVR was more than 200 ml, the patients were recommended to have a CIC. The patients were re-assessed 6 and 12 weeks after the treatment using the Likert scale and OABSS questionnaire.
Statistical analysis
For comparison of baseline, after 6 and 12 weeks following the treatment score in the OABSS and Likert scale of the two treatment groups, continuous variables were analyzed by the Mann-Whitney-Wilcoxon test since groups and parameters were not normally distributed. Fisher’s exact test for count data was used to check the independence between the features described in the columns and rows of Table I. The assumed significance level is α = 0.05. The results were generated using R statistics language [8].
Results
Therapeutic effects
The comparison between the study and the control group pertained to the total OABSS score, together with answers to specific questions 6 and 12 weeks following the treatment. There were no significant differences in total and symptom score at baseline and during follow-up (6 and 12 after treatment) between the two groups (Table II).
Table II
Comparison of the effectiveness of the treatment using the OABSS and Likert scale in the sixth and the twelfth week after treatment
General improvement and reduction of specific symptoms were evaluated according to the Likert scale. Significant improvement was similar (result of 1 or 2 on the Likert scale) and was achieved in 66.7% and 69.2% after 6 weeks and in 63.9% and 64.1% after 12 weeks in the BTX-A + MB group and only-BTX-A group, respectively. Similarly, the Mann-Whitney-Wilcoxon test did not show a statistically significant difference between the groups at 6 and 12 weeks.
Adverse effects
Urinary tract infection developed in 1 (2.8%) and 7 (17.9%) patients receiving BTX-A + MB and only BTX-A, respectively. Urinary retention was observed in 1 (2.8%) and 3 (7.7%) patients receiving BTX-A + MB and only BTX-A, respectively. Considering the total number of patients with complications, 2 (5.6%) vs. 9 (23.1%), there was a significant difference between the two groups (p = 0.049) (Table III).
Table III
Comparison of the total number of complications using Fisher’s exact test. There was significantly less UTI and UR in the group using MB
[i] RIOAB – idiopathic refractory overactive bladder, BTX-A + MB – botulinum toxin + methlyene blue, BTX-A – only botulinum toxin, UTI – urinary tract infection, UR – urinary retention, N – number of counts for the appropriate category, NR – percentage of the number of counts divided by the sum of numbers in the rows for the appropriate category, NC – percentage of the number of counts divided by the sum of numbers in the columns for the appropriate category.
Discussion
Our results show that the combination of BTX-A and MB does not influence the effectiveness of the treatment. Based on major, multicentre studies conducted on large groups of patients, the therapeutic effect of BTX-A in the treatment of RIOAB is assessed at 60–65% [9–11]. We obtained similar results in our study (64.9% for the group with MB vs. 63.2% for the control group in week 12 – patients satisfied and very satisfied on the Likert scale). Similarly, the analysis of the OABSS questionnaire did not show a significant difference between the examined groups either in the overall score or the score of individual symptoms. However, our method may result in additional benefits. In order to exert its therapeutic activity, the toxin must disperse in the tissue. The addition of a color marker may be very helpful in controlling the proper administration of the drug and thus can both ease the procedure for the operator and, consequently, improve its effectiveness. The use of a colored solution allows for intraoperative control of the depth of injection, as well as easy identification of the parts that have not been covered. It may have an impact on less experienced operators. Our modified procedure could be performed more confidently by young urologists during training.
The most commonly observed adverse effects of using BTX-A in RIOAB treatment include urinary tract infection (UTI) and urine retention (UR). The UTI can result from any procedure with the use of an endoscope in the urinary tract – on average, it occurs in 8% (5–15%) of such cases. In the case of administering injections of BTX-A to the bladder, the mucosa is affected by tissue destruction, which increases the frequency of occurrence of UTI to 21.4% with the use of a standard dose of 100 IU of BTX-A [2]. Increased volume of retained urine is yet another factor that may lead to the development of UTI. We found significantly fewer complications (UTI and UR) in the test group 14 days after the procedure. This effect may be attributed to MB, whose bacteriostatic properties are well known [12] – in fact, the substance is successfully applied in modern dressings for slow-healing wounds [13, 14]. The MB within the dressing physically binds with harmful bacterial byproducts (such as endotoxins), an action that may also increase patients’ benefit. As with all living cells, bacterial survival depends on tightly controlled redox stability that balances reductive and oxidative processes (conceptually similar to pH balances) in order to function and thrive. MB alters the redox environment and creates an environment unsustainable for bacterial survival [15, 16].
There are also reports indicating that MB may have neuroprotective properties. MB supports cellular respiration in mitochondria and strengthens synaptic connections, which is considered to lead to better cognitive abilities and memory. The MB acts as an additional electron medium, supporting cellular respiration in mitochondria, which leads to producing more energy available for cellular processes in the form of ATP [17–19]. The MB may be an attractive subject for further clinical trials in the case of various diseases within the range of overactive bladder, in which malfunction of nerve conduction is among possible etiological factors.
The weak point of our study is the small number of participants. The evaluation of the effectiveness of BTX-A therapy in our study was based on the analysis of questionnaires. It seems to be reasonable to repeat the test using an objective biomarker such as urinary nerve growth factor [20].
Conclusions
In our study, we did not prove the advantages of applying a therapy using MB for the effectiveness of treating RIOAB with BTX-A. Limited occurrence of UTI, which is one of the typical possible complications, seems to be an interesting effect which may be of interest in future trials. Perhaps the application of MB or another bacteriostatic substance/drug will allow for limiting the standard perioperative preventive antibiotic treatment. The pleiotropic property of MB seems interesting; however, further research conducted on a larger group of patients is required in order to evaluate the effectiveness of the method and devise a scheme for proper administration of MB.