









Introduction
Menopause is a natural stage of a woman’s life and is accompanied by many physical and emotional changes [1, 2]. The number of postmenopausal women is increasing worldwide. The population of postmenopausal women is expected to reach 1.1 billion by 2025 [3]. During this period, women can experience many symptoms such as hot flashes, night sweats, sleep and mood disorders, loss of memory, lack of concentration, nervousness, depression, complaints related to bones and joints, and decreased bone mass. The severity of these symptoms affects women’s personal and social functioning and quality of life [4, 5]. Psychological and physical complaints during this period cause negative emotions in women.
These affect couples’ relationships and marital adjustment [1]. Marital adjustment indicates the accommodation of couples when interacting with each other [6]. It describes the quality of marital relationships and couples’ marital satisfaction [7] and affects many aspects of their individual and social lives. In proper marital adjustment, a couple often feels happy and satisfied living together [6, 8, 9]. A study by Sis Çelik and Pasinlioğlu showed that marital adjustment decreases with an increase in menopausal symptoms [1]. The partner is the primary emotional support in the life of a postmenopausal woman. During this period, women need more support from their husbands. On the other hand, communication problems in this period can damage women’s quality of life and negatively affect couples’ relationships [10, 11]. Reducing the symptoms of menopause, especially in the psychological field, leads to better relationships for women. Women with higher levels of loneliness and limited communication also experience more severe menopausal symptoms [12, 13]. Communication skills are necessary to build a safe relationship, and they lead to healthy behavior and affect a person’s feelings about themselves and others. Behavioral scientists believe that life skills training is one of the most effective measures to help people have a better and healthier life. It affects people’s self-confidence and self-esteem positively [14]. The transactional analysis (TA) approach, developed by Eric Berne, is one of the methods used to empower and improve the communication of family members [15]. This approach has been very effective in improving relationships and compatibility with others and how humans know themselves [16]. Studies have shown that communication skills training (CST) significantly reduces marital discord [17–19]. Given the gradual aging of the world’s population, it seems that paying attention to the health of this age group can be a step towards improving their quality of life [20, 21]. Due to the changes women feel during the menopausal period and how they affect women’s interpersonal relationships, strengthening communication skills is essential in this period. Therefore, this study was designed and conducted to investigate the effect of CST on marital adjustment in postmenopausal women.
Material and methods
Study design and intervention
The present study had a quasi-experimental, parallel, three-stage design (pre-test, post-test, follow-up).
Transactional analysis is one of the approaches of interpersonal psychotherapy. The therapeutic aim of this theory is to increase the clients’ awareness of their personality structure (child, adult, and parent modes) and interpersonal interactions (complementary and intersecting relationships) to express the concept of conflict, interpersonal incompatibilities, and dissatisfaction with the relationship. Transactional analysis enables people to better know themselves, their thoughts, and emotions. Through this technique, many shortcomings and problems in interpersonal relationships can be identified and solved. Also, with training, participants learn to control their own actions and improve their interpersonal skills [22].
The intervention framework was established based on Eric Berne’s (1996) principles of TA [22, 23], a review of the literature [1, 2, 9, 11, 13, 23–25], objectives of the study, and opinions of the research team (a clinical psychologist, a Ph.D. in reproductive health, and an M.Sc. student in midwifery counseling). The group intervention included eight 90-minute sessions, one session per week (Table 1).
Table 1
Content of communication skills training for marital adjustment in postmenopausal women based on the transactional analysis approach
Sampling, randomization, and study participants
This quasi-experimental study with a parallel design was performed by the availability sampling method.
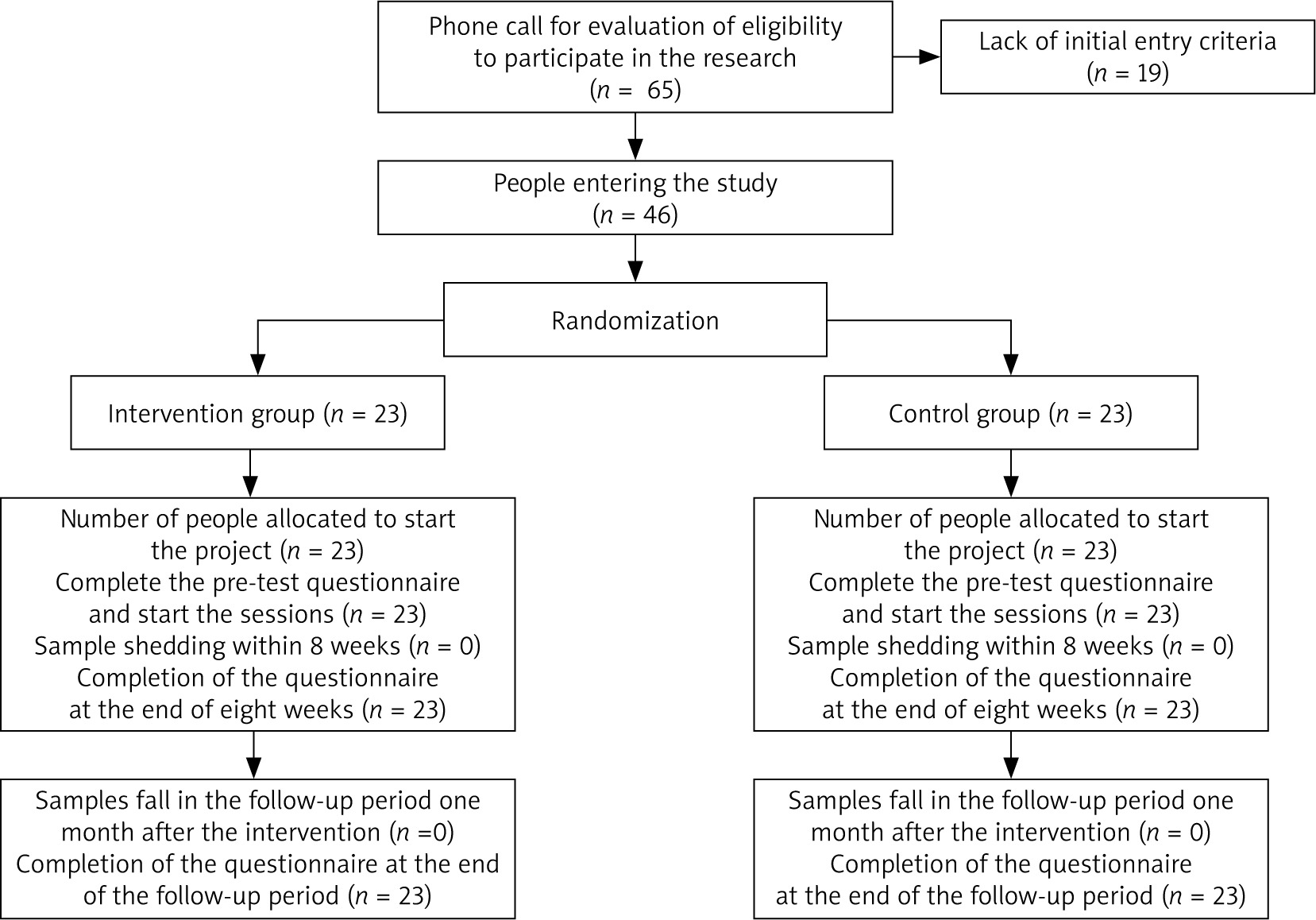
According to the study of Davoudvandi et al. [26], the sample size was estimated to be 46 (23 in each group) by considering the effect size (Cohen effect: 0.81), power of 80%, type II error of 0.20, significance level of 5%, and 20% dropout.
The target group consisted of postmenopausal married women who were referred to Imam Mohammad Taghi Comprehensive Health Center in Isfahan-Iran and were invited to participate in this study by phone. The women had an electronic file at the Comprehensive Health Center, and we invited 46 eligible women to participate in this study by telephone. Participants were randomly assigned to two groups, the intervention group (n = 23) and the control group (n = 23), using a random number table. No one dropped out or was excluded from the study (Fig. 1).
Inclusion criteria
Menopausal married women of Iranian nationality, who were 45- to 60-years-old, could read and write, and were interested in participating in training sessions were included.
Exclusion criteria
Those who were simultaneously participating in another psychotherapy and counseling program, had acute mental-personality disorders (based on the psychiatrist’s diagnosis), substance abuse, or drug abuse, or had faced a severely stressful event in the last six months were excluded.
Dropout criteria
Absence from at least two sessions and encounter with severely stressful events at any stage of the study.
The intervention group received eight communication skills training sessions with a TA approach, and the control group received a routine program. The present study was approved by the local Ethics Committee of Shahid Sadoughi University of Medical Sciences (IR. SSU. REC. 1398.198). Before the study, the objectives of the study were explained to all participants. All participants provided written informed consent. The participants of both groups filled out the questionnaires before, immediately after, and one month after the intervention. Due to the COVID-19 epidemic, training sessions were held in small groups and in compliance with health protocols.
The sessions were conducted by a person trained in TA and CST (second author). The MSc student in midwifery counseling obtained a certificate for communication skills training with the TA approach. She held eight sessions (90 minutes, weekly) under the supervision of a clinical psychologist. For ethical reasons, after the study, the contents of the sessions were summarized for the control group in the form of a training session.
Measurements
Socio-demographic questionnaire: this questionnaire included couples’ age, education level, occupation status, and satisfaction with economic situation.
The dyadic adjustment scale (DAS): marital adjustment was evaluated by Spiner’s DAS. The dyadic adjustment scale is a 32-item tool for assessing the quality of a marital relationship from the viewpoint of one spouse or both. The dyadic adjustment scale includes four dimensions: dyadic consensus, dyadic satisfaction, dyadic cohesion, and affectional expression. The total score of all questions is between 0 and 151. Scores above 100 indicate high marital adjustment. Mehdipour et al. explained the scoring of the questionnaire in their study [27–29]. The dyadic adjustment scale was adapted to Persian by Moosavi (Cronbach’s α 0.90) and Mirghafourvand (intraclass correlation coefficient and Cronbach’s α, 0.90 and 0.85, respectively) [25, 30]. In the present study the reliability of the questionnaire was confirmed through the application of a pre-test and a post-test after 2 weeks, with a Cronbach α of 0.7 and an intraclass correlation coefficient of 0.74.
Queen Dam communication skills questionnaire: Communication skills were evaluated by the Queen Dam communication skills questionnaire. This questionnaire has 34 items describing communication skills. The items are scored based on a 5-point Likert scale (1–5), and the score range is 34–170. Scores of 34–68, 69–102, and 103–170 indicate poor, average, and high communication skills, respectively [31]. The questionnaire was adapted to Persian with a Cronbach’s α of 0.76 [32] and 0.69 [33] for the whole questionnaire, indicating acceptable internal consistency.
The questionnaires were completed before, immediately after, and one month after the training program by both groups.
Data analysis
Data were analyzed with SPSS-22; the Kolmogorov-Smirnov test was used for data normality. The independent t-test, χ2 test, ANOVA, repeated measures ANOVA, and Bonferroni test were used. A p-value < 0.05 was considered statistically significant.
Ethics approval and consent to participate
This study was approved with the ethics code of IR.SSU.REC.1398.198 by the Shahid Sadoughi University of Medical Sciences Research Council in Yazd, Iran. We received written informed consent from study participants after explaining the purpose of the study. The informed consent of illiterate participants (4 persons) was obtained from their daughters. Confidentiality was maintained by omitting participants’ identification information. All stages have been conducted following the Declaration of Helsinki.
Results
The present study showed the normality of demographic characteristics in the two groups. The women in the two groups were not significantly different in socio- demographic characteristics (Table 2).
Table 2
Comparison of demographic characteristics of intervention and control groups
The mean scores of marital adjustment were not significantly different between the two groups before the study (p < 0.05). However, after the intervention and in the follow-up period, a significant difference was observed between the mean scores of marital adjustment of the two groups (p < 0.001). After the intervention, the mean marital adjustment score was significantly higher than the mean score before the intervention (p < 0.001). Also, the trend of changes in marital adjustment scores in the three stages of measurement was different between the two groups (p < 0.001) (Table 3).
Table 3
Comparison of mean and standard deviation of marital adjustment in the two groups
The mean scores of communication skills of the women in the two groups before the study were not significantly different, but after the intervention and in the follow-up period, a significant difference was observed between the mean scores of communication skills of the two groups (p < 0.001) (Table 4).
Table 4
Comparison of mean and standard deviation of communication skills in the two groups
During training sessions, the main concerns expressed by the participants in this period of life (postmenopause) included sleep and mood disorders, nervousness, depression, and joint pain, sexual relationships, communication with the spouse and spouse’s parents, participation in critical decision-making, and household chores.
The participants orally expressed their satisfaction with the impact of this training program on their communication skills. The improvement of the mean scores of communication skills from a medium to a high level reflects this fact.
Discussion
The aim of the present study was to explore the effect of communication skills training with the TA approach on menopausal women’s marital adjustment. Menopause affects women’s physical, sexual, mental, and social health and causes conflict between spouses. Sexual satisfaction and marital adjustment decrease depending on the severity of menopausal symptoms [11, 34, 35]. In the present study, women’s mean marital adjustment scores before the intervention were 52.57 ±4.85 and 52.57 ±4.85 in the intervention and control groups, respectively. In studies conducted in Turkey to investigate marital adjustment in menopausal women, the mean marital adjustment score varied between 104.60 ±32.98 and 92.1 ±11.2 [36, 37]. This difference may be due to differences in socio-demographic features, the intensity of menopausal symptoms, sexual function, cultures, and women’s personalities [34, 36, 37]. The results showed a significant increase in communication skills and marital adjustment scores in the intervention group compared to the control group after the intervention and one month later. This indicates the effectiveness of CST with the TA approach in postmenopausal women. Also, teaching effective verbal and nonverbal communication can facilitate many barriers to proper communication [38]. Group training in reciprocal behavior analysis increases cognitive flexibility. It improves problem-solving, emotional companionship, emotional mating, behavior control, and efficiency in women with marital disputes [39, 40]. Behavioral-communication skills training has also been effective in increasing couples’ marital adjustment and sexual intimacy [41]. There is a significant relationship between communication skills and marital intimacy. Communication skills are strong predictors of marital intimacy [42, 43]. Communication skills affect almost all aspects of marital life [44]. Communication skills training will probably allow spouses to find each other’s child ego state (under supervision of the adult ego state), caress each other, and become more intimate with each other. Communication skills training based on the TA approach has helped increase the intimacy of spouses [45].
Conclusions
Communication skills training with a TA approach in postmenopausal women increases marital adjustment. Therefore, considering the effects of menopause on marital adjustment in postmenopausal women and the need for the strengthening of marital adjustment, it is suggested that midwives use this method as an effective way to improve the lives of postmenopausal women in comprehensive health centers.