

Purpose
Cervical cancer is the fourth most commonly diagnosed cancer and the fourth leading cause of cancer-related deaths in women, with an estimated 604,000 new cases and 342,000 deaths worldwide in 2020 [1]. External beam radiotherapy (EBRT) with concurrent chemotherapy combined with brachytherapy has been the standard of care for locally advanced cervical cancer [2]. Although EBRT has made significant advancements, brachytherapy remains irreplaceable, as it is a crucial factor in achieving a higher local control (LC) rate and long-term outcomes [3, 4]. In traditional two-dimensional (2D) brachytherapy, dose points were used to assess radiation doses delivered to tumors and organs at risk (OARs). The introduction of three-dimensional (3D) image-guided brachytherapy has marked the beginning of a new era in brachytherapy of cervical cancer. For image-guided brachytherapy, GEC-ESTRO published recommendations providing a common language to describe target concepts, therefore, both volume and point doses can be used to evaluate the radiation exposure to tumors and critical OARs [5, 6]. Gross target volume (GTV) represents the macroscopic tumor extension detected by clinical examination and visualized on magnetic resonance imaging (MRI). High-risk clinical target volume (HR-CTV) signifies the entire cervix and presumed extra-cervical tumor extension. Intermediate-risk clinical target volume (IR-CTV) denotes the microscopic tumor load, initial GTV as superimposed on the topography at the time of brachytherapy, and safety margin surrounding HR-CTV. D100, D98, and D90 provide evaluations of the minimum dose, near minimum dose, and more stable peripheral dose to targets. The integration of MRI has made the delineation of target volumes and OARs more precise, resulting in more accurate dose evaluation in brachytherapy. The improvement of accuracy in dose assessment increases the possibility of establishing meaningful and accurate dose-effect relationship (DER) to ensure optimized treatment outcomes for patients undergoing brachytherapy.
In radiotherapy, the establishment of DER and clinical validation based on DER results have led to more appropriate and optimized prescription dose in radiotherapy [7, 8]. In radical radiotherapy for cervical cancer, there are significant DERs between the tumor control rate or probability of normal tissue side effects versus doses [7-10].
The current study aimed to identify the DERs of EBRT combined with brachytherapy for cervical cancer, and attempted to show the direction of future research in DER. Also, the study provided dosimetric references, which could be implemented in clinical practice.
Material and methods
Data sources and search strategies
A comprehensive literature search was performed using the PubMed, Web of Science, and Cochrane Library databases to identify full articles reporting DERs for clinical end-points or OARs toxicity in cervical cancer radical radiotherapy. MeSH term ‘‘Uterine Cervical Neoplasms’’, and all entry terms in title or abstract were used to identify articles on cervical cancer. Next, the following subject categories in title or abstract were searched: “Dose Effect”, “Dose-Volume Response”, “Dose Predicts”, “Dose-Volume Correlation”, “Dose Response”, “Probit Model Analysis”, and “Dose Toxicity”; intersection with articles on cervical cancer was considered (Supplementary Table 1). The last search of this systematic review was performed on Jan 20, 2023.
Inclusion criteria
1. The topic of articles was EBRT with concurrent chemotherapy combined with brachytherapy for cervical cancer.
2. Cumulative equivalent dose in 2 Gy per fraction (EQD2) of EBRT and brachytherapy was considered, including dose-volume histogram parameters and/or point doses to target volumes and/or OARs.
3. For volume-based studies, the delineation of target volumes and OARs needed to comply with GEC-ESTRO recommendations [5, 6].
4. Dose-response or dose-toxicity examinations based on a single cohort or regression analysis using XLSTAT or statistical analysis system (SAS) of multiple published data were considered.
5. Dose-response relationships or dose-toxicity relationships were significant at p < 0.05.
Exclusion criteria
1. External beam radiotherapy that adopted proton beam or heavy ion beam.
2. For radiation dose boost in residual disease after EBRT, articles related to techniques other than brachytherapy, such as stereotactic body radiotherapy (SBRT) were excluded, since they were used as second-line treatment options.
3. Relevant factors, other than dose, such as age, tumor volume, overall treatment time, smoking, human papillomavirus infection, etc., affecting clinical end-points or toxicity in DER.
4. Treatment combined with other modalities, such as surgery, hyperthermia, immunization, and targeted therapy.
5. Articles including techniques with midline block and/or parametrial boost.
6. Due to the language barriers, non-English articles were excluded.
Data extraction
After deleting duplicates, the articles were screened by title and abstract, and then by full text. Literature screening and data extraction were performed independently by two authors according to the inclusion and exclusion criteria, and objections were resolved through negotiations. For single cohort studies, if data originated from overlapping or almost the same patients, the most recent and comprehensive information were included.
The following data were extracted from the included studies: first author, year of publication, year of treatment, number of patients, age, FIGO stage, brachytherapy modality, median follow-up time, dose parameters, clinical end-points or side effects, significance (p-value), estimated dose at 90% (ED90) in DERs or estimated dose at x% (EDx) in dose-toxicity relationships, and data from a single cohort or multiple studies. When ED90 or EDx were not available, dose-effect curve was used to obtain the parameters. The process of obtaining ED90s or EDxs was cross-checked by two authors. For DERs between the same dose parameter and the same clinical end-point or the same OAR toxicity, in order to intuitively compare them from different authors, coordinates of the curves from the articles were extracted, dose-effect curves were reconstructed, and placed in the same coordinate system. Coordinates of DERs were obtained using Paint (from Windows, Microsoft, WA, USA), and their reconstructions were performed using Excel (Microsoft, WA, USA).
Results
Description of included studies
A total of 1,445 potentially related studies were identified using the systematic literature retrieval strategy. After deleting duplicates, 30 DERs studies were obtained through the title, abstract, and full-text screening, including 11 dose-response relationships for tumor control and 19 dose-toxicity relationships for OARs, as shown in Suppl. Fig. 1.
The main characteristics of dose-response relationships for tumor control are presented in Table 1 [7, 11-20]. The most used dose parameters for predicting tumor control were HR-CTV (n = 9), followed by IR-CTV (n = 5) and GTV (n = 3). The most used clinical end-points were LC (n = 10), followed by overall survival (OS, n = 2), progression-free survival (PFS, n = 1), and cancer-specific survival (CSS, n = 1). The main characteristics of dose-toxicity relationships for OARs are shown in Table 2 [9, 21-38]. The most used dose parameters for predicting toxicity were D2cc of rectum (n = 8), followed by D2cc of bladder (n = 5), dose to International Commission on Radiation Units and Measurements (ICRU) rectum reference point (Dicru, n = 4), and D1cc of rectum (n = 4). The most common OARs to be analyzed for dose-toxicity were rectum (n = 11) and colorectal (n = 11), followed by bladder (n = 5), vagina (n = 3), and urethra (n = 1).
Table 1
Dose-effect relationships between dose and tumor response
| Author, year [Ref.] | Years of treatment | No. of patients | Age, years (range) | FIGO stage | BT modality | Median follow-up time (months) | Dose parameter | Clinical end-point | p-value | ED90 (95% CI) (GyEQD2,10) | Source of data |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Dimopoulos, 2009 [11] | 1998-2003 | 141 | 60 (26-92) | I-IVA | MR-based IC/IS BT, HDR | 51 | HR-CTV D90 | LC | 0.005 | 86 (77-113%) | Single cohort |
| Dyk, 2014 [12] | 2007-2011 | 134 | 49 (25-85) | IB1-IVB | MR-based IC BT, HDR | 29 | GTV D100 GTV D90 GTV Dmean | LC | < 0.001 < 0.001 < 0.001 | 69 (60-85%)* 98 (85-121%)* 260 (218-370%)* | Single cohort |
| Mazeron, 2015 [7] | 2006-2011 | 225 | 48.5 ±11.2 | IB1-IVA | 3D IC/IS BT, PDR | 39 | HR-CTV D90 IR-CTV D90 | LC | 0.024 0.004 | 83.5 (76.5-102.6%) 70.8 (65.4-111.9%) | Single cohort |
| Mazeron, 2016 [13] | N.A. | 1,299 873 | N.A. | N.A. | 3D-BT, HDR | N.A. | HR-CTV D90 IR-CTV D90 | 2/3-year LC 2/3-year LC | < 0.0001 0.009 | 81.4 (78.3-83.8%) 69.2 (67.2-78.1%) | 13 articles 7 articles |
| Tanderup, 2016 [14] | 1998-2009 | 280** 141*** 280** 141*** | 54 (23-91) | IB-IVB | 3D IC/IS BT, HDR, or PDR | 46 (1-164) | HR-CTV D90 HR-CTV D90 GTV D100 IR-CTV D90 | LC | 0.022 0.008 0.006 0.025 | 74.9 92.6 77.5 73.6 | Retro-EMBRACE |
| Zhang, 2019 [15] | 2010-2018 | 110 | 23-84 | IB2-IVA | 3D IC/IC BT, HDR | 72.3 | HR-CTV D100 HR-CTV D100 HR-CTV D98 HR-CTV D98 HR-CTV D98 HR-CTV D90 | OS CSS OS CSS LC OS | < 0.001 0.004 < 0.001 0.003 0.034 0.001 | 76.0 (72.6-84.7%) 75.6 (71.5-90.7%) 86.8 (82.4-98.7%) 85.6 (80.7-101.7%) 78.6 (64.2-103.4%) 100.4 (94.5-118.9%) | Single cohort |
| Tang, 2020 [16] | N.A. | 2,893 1,172 | N.A. | N.A. | 3D BT | N.A. | HR-CTV D90 IR-CTV D90 | LC | < 0.0001 0.464 | 83.7 (80.6-87.8%) 69.3 (64.2-237.3%) | 33 articles 8 articles |
| Li, 2021 [17] | N.A. | 520 | N.A. | N.A. | 3D IC/IS BT | N.A. | HR-CTV D90 | LC | 0.030 | 88.8 (84.1-102.8%) | 12 articles |
| Ke, 2022 [18] | 2014-2019 | 93 | 53.5 ±10.2 | IB2-IVA | N.A. | 19.6 (2.6-60.7) | GTVres D98 GTVres D98 GTVres D100 GTVres D100 | 2-year OS 2-year PFS 2-year OS 2-year PFS | 0.031 0.020 0.022 0.010 | 129.1 (112.1%) 152.2 (127.9%) 113.5 (100.3%) 127.1 (112.0%) | Single cohort |
| Li, 2022 [19] | N.A. | 3,616 881 | N.A. | N.A. | 3D BT | N.A. | HR-CTV D90 IR-CTV D90 | LC LC | < 0.001 0.003 | 79.1 (69.8-83.7%) 66.5 (62.8-67.9%) | 19 articles 7 articles |
| Schmid, 2023 [20] | 2008-2015 | 1,318 | N.R. | IB1-IVA | 3D IC/IS BT | 52 | HR-CTV D90 | LC | < 0.050 | **** | EMBRACE |
[i] FIGO – International Federation of Gynecology and Obstetrics, BT – brachytherapy, ED90 – estimated dose at 90%, CI – confidence interval, D90/100 – minimum doses delivered to 90%/100% of the target volume, Dmean – mean dose, MR – magnetic resonance, IC/IS – intra-cavitary and interstitial, HDR – high-dose-rate, LC – local control, PDR – pulsed-dose-rate, GTVres – residual gross tumor volume, N.A. – not applicable, OS – overall survival, CSS – cancer-specific survival, PFS – progression-free survival, N.R. – not reported, *95% CI read from figure, **sub-group: stage II, ***sub-group: stage III + IV, ****HR-CTV D90 85 Gy led to 95% (95% CI: 94-97%) 3-year local control for squamous cell carcinoma histology in comparison with 86% (95% CI: 81-90%) for adeno/adenosquamous carcinoma histology
Table 2
Dose-effect relationships between dose and toxicity of organs at risk
| Author, year [Ref.] | Year of treatment | No. of patients | Age, years (range) | FIGO stage | BT modality | Median follow-up time (month) | Dose parameter | OAR toxicity | p-value | EDx (GyEQD2,3) | Source of data |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Clark, 1997 [21] | 1988-1991 | 43 | N.R. | N.R. | 2D IC BT, HDR | 51 | Rectal Dicru | Rectal complication G3-4 | 0.003 | ED10/26: 157/207 | Single cohort |
| Sakata, 2002 [22] | 1987-1999 | 105 | 66 (36-88) | IA-IVB | 2D IC BT, HDR | 63 | Max rectal dose | Late rectal complications | – | ED5/50: 64/79 | Single cohort |
| Koom, 2007 [23] | 2004-2005 | 71 | 56 (23-77) | IB-IIIB | CT-based IC BT, HDR | 12 (minimal) | Rectal D2cc Rectal D1cc Rectal Dicru | Sigmoidoscopy score G ≥ 2 | 0.020 0.020 0.030 | ED20: 53 ED20: 54 ED20: 47 | Single cohort |
| Georg, 2009 [24] | 1998-2004 | 35 | 57 (29-82) | IB-IVA | MR-based IC/IS BT, HDR | 18 | Rectal D2cc Rectal D1cc Rectal D0.1cc Rectal Dicru | Rectal G ≥ 2* Rectal G ≥ 2* Rectal G ≥ 2* Rectal G ≥ 2* | 0.0046 0.0080 0.0427 0.0258 | ED5/10/50: 64.7/65.3/75.8 ED5/10/50: 66.7/67.5/83.3 ED5/10/50: 68.0/70.3/113.1 ED5/10/50: 63.9/65.3/92.5 | Single cohort |
| Georg, 2012 [9] | 1998-2003 | 141 | N.R. | N.R. | MR-based BT, HDR | 51 | Rectal D2cc Rectal D1cc Bladder D2cc Bladder D1cc Bladder D0.1cc | Rectal G 2-4* Rectal G 2-4* Bladder G 2-4* Bladder G 2-4* Bladder G 2-4* | 0.0178 0.0352 0.0274 0.0268 0.0369 | ED5/10/20: 67/78/90 ED5/10/20: 71/87/90 ED5/10/20: 70/101/134 ED5/10/20: 71/116/164 ED5/10/20: 61/178/305 | Single cohort |
| Kim, 2013 [25] | 2004-2006 | 77 | N.R. | IB-IIIB | 3D IC BT, HDR | 70.8 (24-84) | Rectosigmoid colon D2cc | RMC G ≥ 3*** LRC G ≥ 2*** | 0.002 0.005 | ED10/20: 55/66 ED10/20: 57/69 | Single cohort |
| Mazeron, 2015 [26] | 2005-2011 | 217 | 48.3 ±11.7 | IB1-IIIB | 3D IC BT, PDR | 35 (3.3-112.6) | Bladder D2cc Rectal D2cc | Bladder G 2-4** Rectal G 2-4** | < 0.005 < 0.005 | ED10: 68.5 ED10: 65.5 | Single cohort |
| Mazeron, 2015 [27] | N.R. | 69 | 50.2 (27-80) | IB-IVA | 3D IC BT, PDR | 39.1 | Bladder D2cc | Bladder G 2-4** | 0.017 | ED5/10/20: 66.9/72.5/79.4 | Single cohort |
| Mazeron, 2016 [28] | N.R. | 960 | 50.5 ±13.1 | IA-IVA | MR-based BT | 25.4 (3-75.6) | Rectal D2cc | Rectal G 2-4** | < 0.0001 | ED10: 69.5 | EMBRACE |
| Zhou, 2016 [29] | 2008-2009 | 144 | 52 (27-74) | IB2-III | CT-based IC/IS BT | 58 (5-71) | Rectal D2cc | Rectal G ≥ 3 | 0.005 | ED5/10/20: 72.0/73.5/75.4 | Single cohort |
| Kirchheiner, 2016 [30] | N.R. | 630 | 49 (22-89) | IB-IVB | 3D IC/IS BT | 24 (IQR, 12-36) | RV-RP | Vaginal stenosis G ≥ 2** | 0.003 | ED16/20/27/34/43: 55/65/75/85/95 | EMBRACE |
| Ujaimi, 2017 [31] | 2008-2013 | 106 | N.R. | IB-IVA | MR-based BT, PDR | 44 (4-76) | Rectal D2cc Bladder D2cc Rectal V55 | Rectal G 2-3 Bladder G 2-3 Rectal G 2-3 | < 0.050 | ED10: 59 ED10: 62 ED10: 4 cc | Single cohort |
| Jensen, 2021 [32] | 2008-2015 | 1,199 | 49 (22-91) | IV-IVB | 3D IC/IS BT, HDR or PDR | N.R. | V43 Gy V57 Gy*** | Diarrhea G 2-4 | < 0.050 | ≤ 2500 cc: 9.5% ≥ 3000 cc: 14.0% ≤ 165 cc: 9.4% ≥ 165 cc: 19.0% | EMBRACE I |
| Rodriguez-Lopez, 2021 [33] | 2007-2017 | 242 | 52 (43-54) | IB1-IVA | MR-based IC/IS BT | 35.8 (IQR, 19-61) | Ureteral D0.1cc | Ureteral Stenosis G ≥ 3** | < 0.050 | ED5/10: 79/90 | Single cohort |
| Spampinato, 2021 [34] | N.R. | 1,153 | 49 (21-91) | IB-IVA | 3D BT, HDR or PDR | 48 (3-120) | Bladder D2cc | 4-y bladder cystitis G ≥ 2** 4-y bladder bleeding G ≥ 2** | < 0.050 | **** | EMBRACE |
| Zhang, 2021 [35] | 2010-2018 | 110 | 54 ±11.0 | IB2-IVA | 3D IC/IS BT, HDR | 72.3 | Rectal D1cc Rectal D1cc Rectal D1cc Rectal D0.1cc | 1-y rectal G 2-4 ***** 3-y rectal G 2-4 ***** 5-y rectal G 2-4 ***** 1-y rectal G 2-4 ***** | 0.001 0.002 0.005 0.015 | ED10: 74 ED10: 67.5 ED10: 67.4 ED10: 83.0 | Single cohort |
| Dankulchai, 2022 [36] | N.R. | 97 | 60 (33-86) | IB2-IVA | 3D IC/IS BT | 20 | PIBS+2 PIBS-2 D+5 | Vaginal stenosis G3** | 0.005 0.005 0.046 | ED15/20: 57.4/111 ED20: 7 ED10/15/20: 52.5/66.6/78 | Single cohort |
| Wang, 2022 [37] | 2016-2018 | 351 | 50 (31-60) | IB-IVB | 2D BT | 38 | Rectal Dicru | Vaginal stenosis G ≥ 2** | < 0.001 | ED21/30/39: 75/85/95 | Single cohort |
| Westerveld, 2022 [38] | 2008-2015 | 301 | 54 (IQR, 43-64) | I-IVA | 3D IC/IS BT, HDR or PDR | 49 | RV-RP PIBS+2 PIBS PIBS-2 VRL | Vaginal stenosis G ≥ 2** | < 0.050 | ≤ 60 Gy: 8.0% ≤ 49 Gy: 10.0% ≤ 15 Gy: 9.0% ≤ 3 Gy: 12.0% ≥ 65 mm: 13.0% | EMBRACE I |
[i] FIGO – International Federation of Gynecology and Obstetrics, BT – brachytherapy, OAR – organ at risk, EDx – estimated dose at x%, N.R. – not reported, IC/IS – intra-cavitary and interstitial, HDR – high-dose-rate, PDR – pulsed-dose-rate, Dicru – ICRU point dose, G – grade, D2cc/1cc/0.1cc – minimum dose to 2 cc/1 cc/0.1 cc volume of organ at risk that received maximum dose, MR – magnetic resonance, RMC – recto-sigmoid mucosal change, LRC – late rectal complication, RV-RP – recto-vaginal reference point, PIBS+/-2 – 2 cm proximal/distal to posterior-inferior border of the symphysis; D+5 – 5 mm below the mucosa in the dorsal point at plane of vaginal top, VRL – vaginal reference length, *late effects in normal tissue/subjective, objective, management, analytic (LENT/SOMA), **common terminology criteria for adverse events (CTCAE), ***lymph node boost, ****for G ≥ 2 bleeding, an increase from < 75 Gy to > 90 Gy in D2cm3 resulted in an increase in 4-year actuarial estimate from 1.5% to 7.5%. For G ≥ 2 cystitis, an increase from 75 Gy to 80 Gy resulted in an increase from 8% to 13%, *****the Radiation Therapy Oncology Group criteria
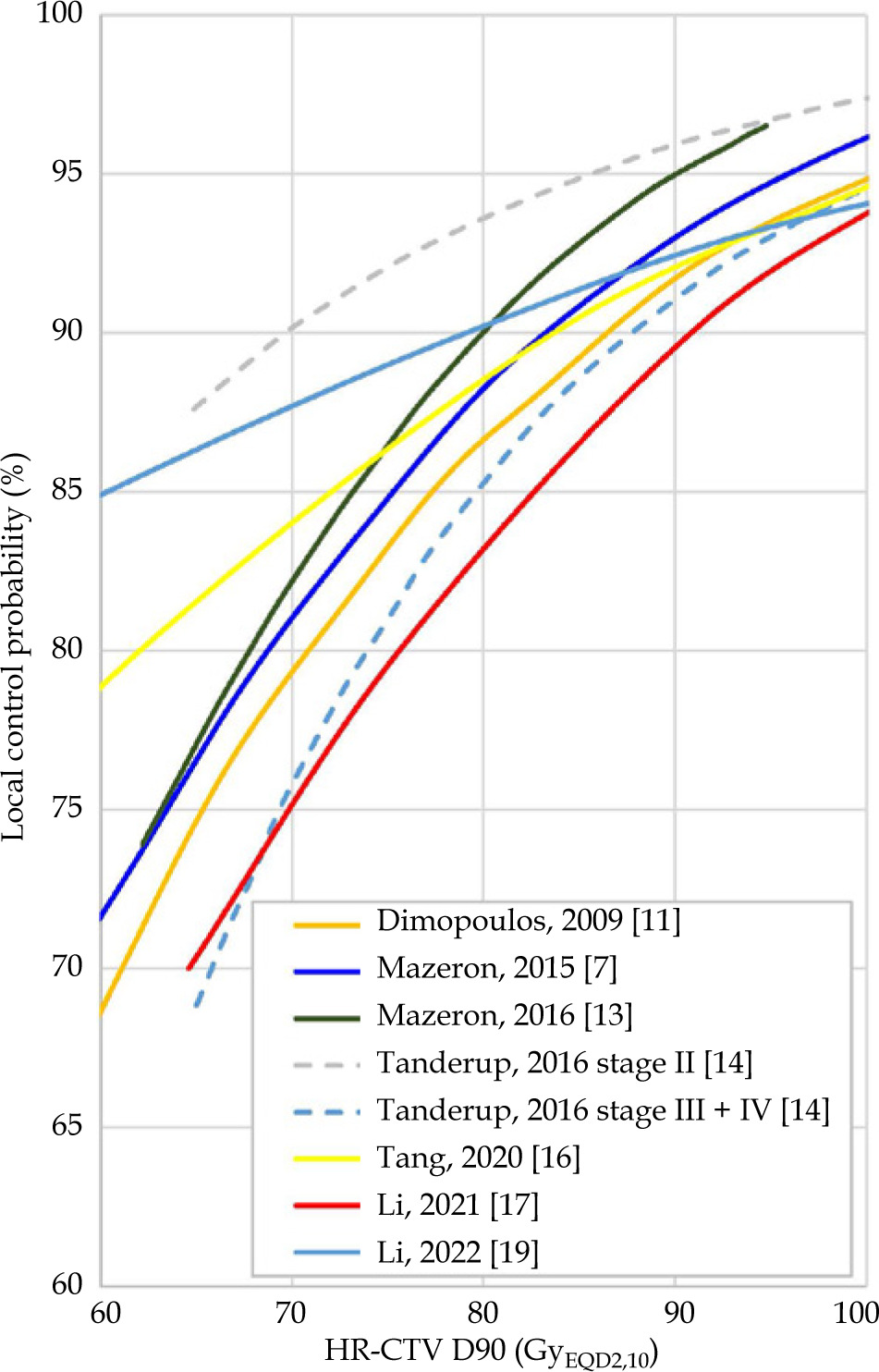
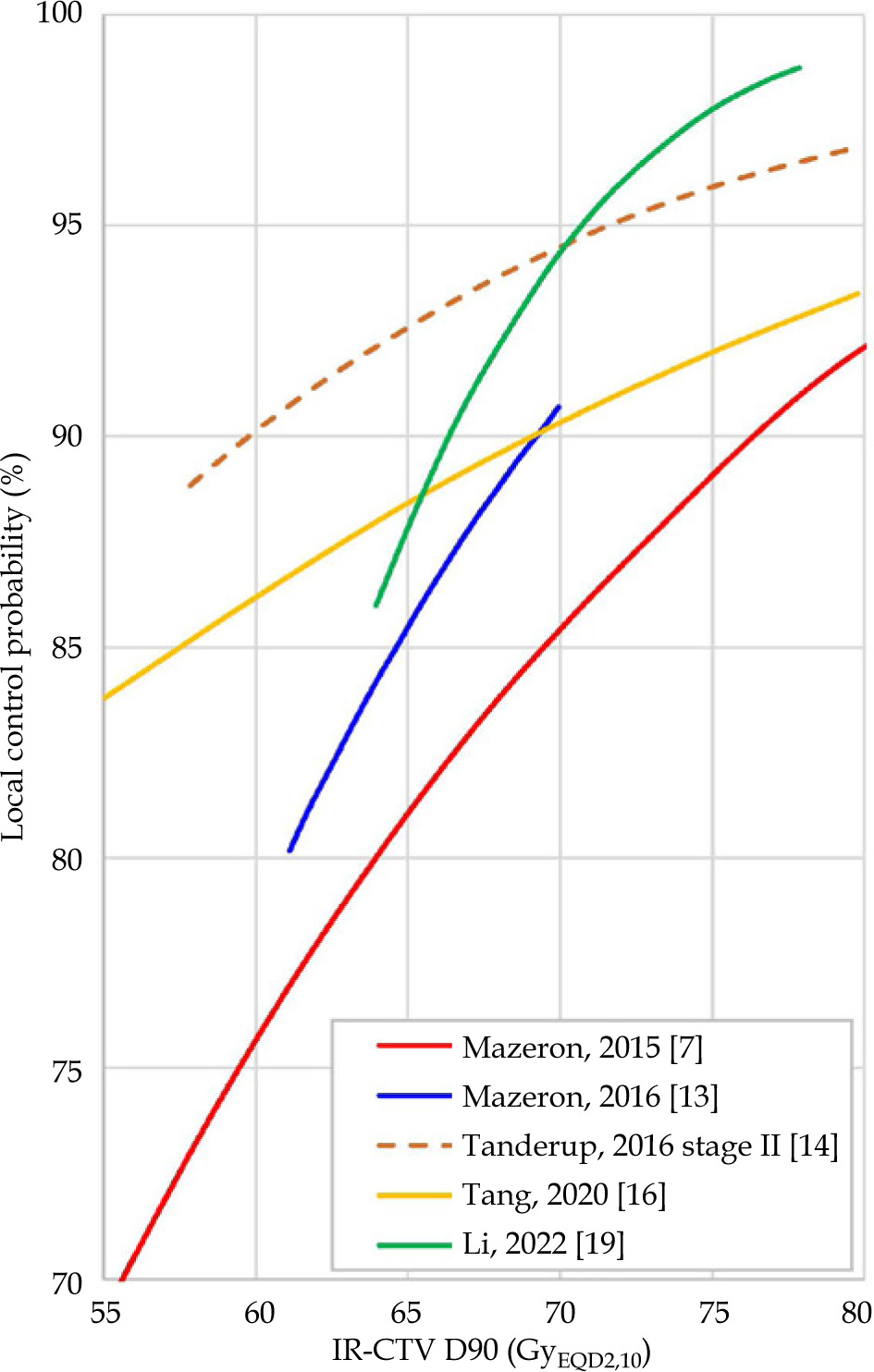
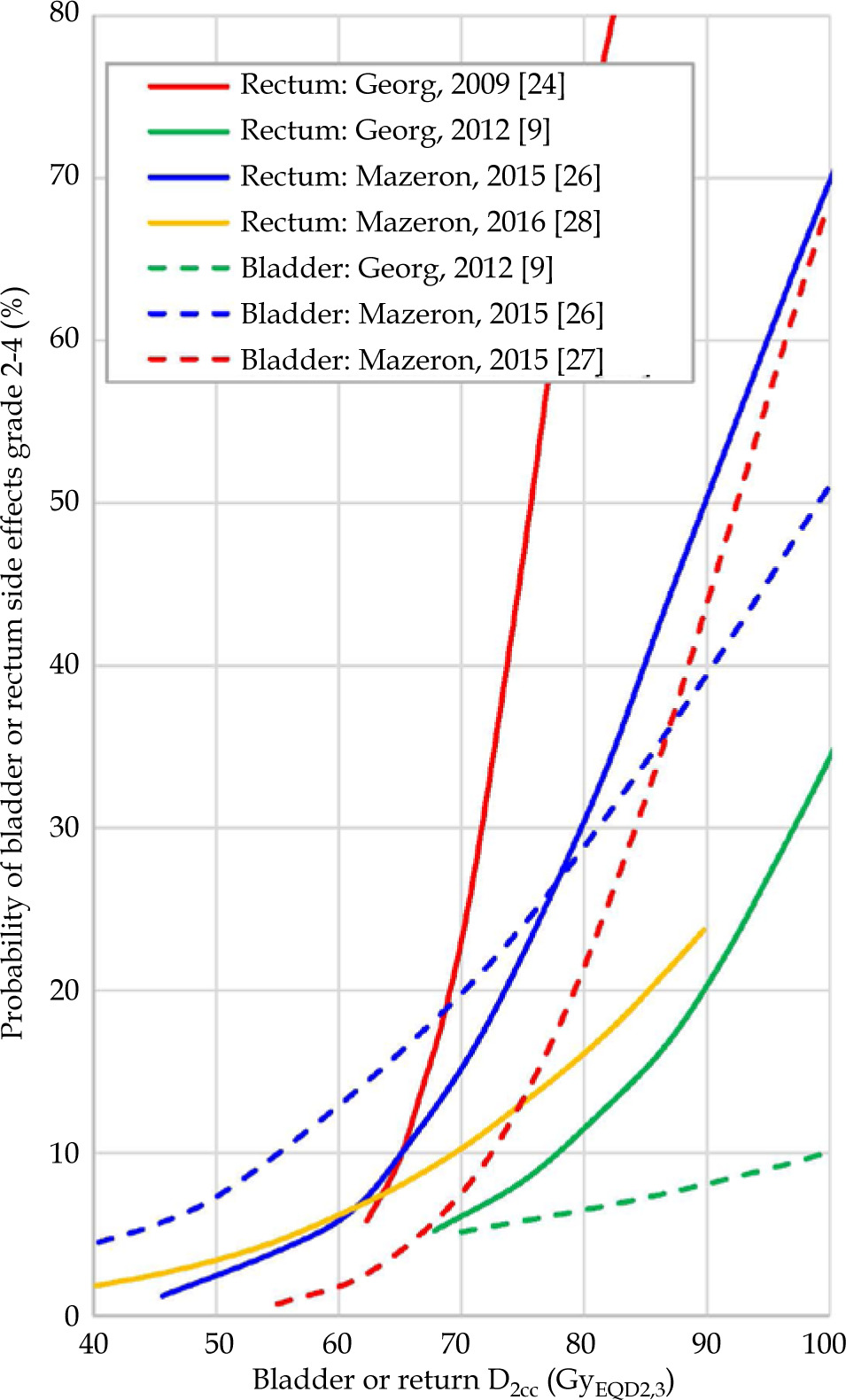
The most common dose-response relationships between the same dose parameter and the same clinical end-point were HR-CTV D90 vs. tumor LC (n = 8), followed by IR-CTV D90 vs. tumor LC (n = 5). To intuitively compare the relationship between different dose-response curves, the coordinates of the curve from the article were extracted, the dose-response curves were reconstructed, and placed in the same coordinate system (Fig. 1 and 2). For dose-toxicity relationships, the most common dose-toxicity relationships between the same dose parameter and the same OAR toxicity were rectal D2cc vs. rectal grade 2-4 late side effects (n = 4), followed by bladder D2cc vs. bladder grade 2-4 (n = 3) (Fig. 3).
Discussion
In radiotherapy, DERs are objective and widely recognized. These relationships show the optimal prescription doses in different types of cancer. For example, in EBRT of prostate cancer, the dose-response relationship can be helpful to determine the optimal prescription dose. Similarly, in stereotactic body radiotherapy (SBRT) for lung cancer, DERs suggest the optimal bio-equivalent dose. In case of EBRT combined with brachytherapy for cervical cancer, DERs guide the prescription dose for target volumes and dose constraints for OARs.
Dimopoulos et al. [11] analyzed the dose parameter and local control (LC) data of 141 cervical cancer patients using SAS software. They found a significant DER between the dose and LC rate in cervical cancer radiotherapy. Specifically, HR-CTV D100 and D90 showed significant dose dependence in local recurrence in all patients as well as in specific sub-groups based on tumor size. This study showed that tumor control rates of > 90% could be expected at HR-CTV D100 > 67 GyEQD2,10 and D90 > 86 GyEQD2,10, respectively. This was almost the first study on dose-response relationship of the target volume in radical radiotherapy for cervical cancer. Furthermore, it laid the foundation for dose constraint in the current EMBRACE II study. Since then, radiation oncologists gradually considered the importance of DERs, and conducted series studies.
To facilitate pooling of clinical data from multiple studies, meta-regression analyses were used to obtain DERs based on numerous patients. These analyses deemed the average or median dose reported in each study, and weighed the observations based on patient number in each research [13, 16, 17, 19].
Figure 1 display eight dose-effect curves for HR-CTV D90 and local tumor control. These curves show similar trends, and a mean local tumor control rate of 90% (range, 86.6-93.0%) can be expected at HR-CTV D90 85 GyEQD2,10 without considering two-subgroup data. Moreover, tumor control rates of 90% can be predicted at HR-CTV D90 from 79.0EQD2,10 Gy to 90.8 GyEQD2,10. These results almost fell within dose constraints of HR-CTV D90 in the EMBRACE II study, ranging from 85 Gy to 95 Gy [39]. The EMBRACE study revealed that many patients with small HR-CTV volumes received high-dose (> 95 GyEQD2,10) treatment, but the local control rate increased only from 95% (85 GyEQD2,10 - 95 GyEQD2,10) to 96%. This can be clearly seen from the decrease in the slope of high-dose range in the dose-response curve.
In addition to the dose-related factors, the efficacy of radical radiotherapy for cervical cancer is influenced by various clinical factors, including pathology of cancer [20], FIGO stage [14], HR-CTV volume at brachytherapy, uterine invasion or not, concurrent chemotherapy or not during EBRT, total treatment time, age at diagnosis, lymph node metastasis or not, etc. [7, 8, 40]. Considering these factors, future dose-effect studies should aim at minimizing the confounding factors to derive specific DERs for different sub-groups of patients.
Similarly, DERs of OARs can help predict the probability of side effects, and can be used as dose constraints in clinical practice. However, it is important to consider potential position drifts in the calculated absorbed dose of OARs between fractions. Among various metrics for dose constraints, D2cc shows greater predictive value due to its lower likelihood of volume deviation compared with D0.1cc and D1cc. For instance, a rectal D2cc of 65-78 GyEQD2,3 can be expected at 10% of grade 2-4 rectal side effects.
Since the vagina is adjacent to the cervix in terms of anatomical position, and vaginal applicator is placed in the vagina between the bladder and rectum, the absorbed dose of the vagina is not evenly distributed. This non-uniformity of dose distribution poses a challenge in accurately assessing the dose delivered to the vagina during brachytherapy. To address this issue, Westerveld et al. [41] proposed the use of 11 vaginal dose reference points to evaluate the dose distribution within the vagina. These reference points were specifically chosen to account for the dose heterogeneity in different regions of the vagina. In a study by Dankulchai et al. [36], data of 97 patients were analyzed to investigate the relationship between dose and side effects of grade 3 vaginal stenosis. It was found that 3 reference points, 2 cm proximal/distal to the posterior-inferior border of the symphysis (PIBS ±2), and 5 mm below the mucosa in the dorsal point at the plane of the vaginal top (D+5), had a significant dose-toxicity relationship with vaginal stenosis. This finding highlighted the importance of accurately assessing the dose delivered to these specific regions of the vagina to predict and control potential side effects. On a lateral radiograph, the ICRU rectum reference point is located on a line drawn from the lower end of intra-uterine source (or from the middle of intra-vaginal source). The ICRU rectum reference point is situated 5 mm behind the posterior wall of the vagina. This point was originally established as a monitoring reference point for rectal dose; however, a research by Kirchheiner et al. [30] indicated that this point can be also used as a dose reference point for evaluating the risk of vaginal stenosis or shortening. Therefore, it was also known as the ICRU recto-vaginal point. This finding underscored the importance of incorporating point dose assessment, particularly at this specific reference point, in the era of three-dimensional brachytherapy. Therefore, a comprehensive evaluation of vaginal dose distribution is necessary due to the anatomical proximity of the vagina to the cervix as well as the uneven distribution of absorbed dose within the vagina.
These significant DERs helped to establish the recommended dose constraints, ensuring that target volumes receive adequate radiation dose while minimizing potential harm to OARs. By adhering to these dose constraints, clinicians can provide safe and effective treatments to patients. Some dose limits or planning aims of the EMBRACE II study are derived from previous significant DERs [39].
In the current study, there were several limitations. Firstly, the study did not include articles published in the last year. Secondly, the included articles used different brachytherapy modes, such as 2D brachytherapy, CT-based 3D brachytherapy, and MRI-based 3D brachytherapy as well as different dose parameters, clinical outcomes, and toxicities, making it difficult to integrate them. Thirdly, studies from 1997 to 2023 were included, and represented an older era of standards of care in imaging, radiotherapy, brachytherapy, and chemotherapy. These potential confounding factors is another limitation of this study. Finally, for aggregated meta regression analysis data from multiple research, overlapping studies could not be eliminated.
Conclusions
In the radical radiotherapy of cervical cancer, there are significant DERs for target volumes and OARs. Due to the establishment of DERs and clinical application based on the results of DERs, the dose constrains of radiotherapy can be more personalized and tailored. Several studies clearly demonstrated that tumor size, histology, and overall treatment time significantly changed the clinical outcomes [7, 8, 42]. Furthermore, considering the interference of these factors, DERs for sub-group patients after excluding confounding factors can provide precise and individualized dose constraints of radiotherapy for cervical cancer in the future.