







Introduction
Achalasia is characterized by the degeneration of inhibitor neurons that are involved in the phasic relaxation of the lower esophageal sphincter (LES). Achalasia is reported with no gender differences around the world and occurs at all ages, ranging up to one person in 100 000 person-years [1]. With the development of endoscopic techniques, peroral endoscopic myotomy (POEM), first reported by Inoue in 2010 [2], has become a mature and efficacious option due to its minimally invasive approach. Previous studies have demonstrated the effectiveness of POEM in the short and medium term, which shows satisfactory results in over 80% of patients [3–5].
Many patients have neuropsychological disorders such as anxiety and depression before surgery. During the perioperative period, they are also affected by surgery and anesthesia, resulting in a strong stress response. POEM is safe and efficient, but there are also serious main adverse events associated with POEM including pneumothorax, gastroesophageal reflux disease, pneumoperitoneum, mucosal injury, hemorrhage, subcutaneous emphysema, mediastinal emphysema, pleural effusion, atelectasis and infection [6, 7]. Postoperative pain is also an adverse event of patients after POEM, and is one of the most unpleasant experiences, which affects patient recovery and prolongs hospital stay [8, 9]. Although many aspects of POEM are increasingly becoming standardized, perioperative managements are still being debated. Therefore, establishing a perioperative protocol is vital to promote recovery and decrease complications of patients undergoing POEM.
In recent years, a strategy of Enhanced Recovery After Surgery (ERAS) has been proposed to integrate minimally invasive surgery, anesthesia, analgesia, to accelerate postoperative recovery, reduce surgical stress and postoperative complications according to evidence based medicine [10]. At present, this concept has been used in several general surgery [11, 12], but it has not been fully developed in endoscopic surgery. Moreover, there is still no evidence for ERAS in POEM and at present no consensus on the clinical pathway has been established. Therefore, it is necessary to improve the perioperative management to promote rapid recovery after surgery and increase the quality of life of patients.
Aim
We aimed to study the safety and effectiveness of an ERAS protocol on the standard postoperative length of stay (LOS) and QoR-15 (Quality of Recovery) score of patients undergoing POEM.
Material and methods
Study design
This was a prospective, randomized pilot study. All procedures were performed at the Zhongshan Hospital (Shanghai, China) from October 2017 to March 2018. The study was approved by the Ethics Committee of Zhongshan Hospital on 29 August 2017 (approval number B2017-114R) and conformed to the provisions of the Declaration of Helsinki in 1995 (as revised in Edinburgh 2000). All patients provided written informed consent. The trial was registered at the Chinese Clinical Trial Registry (ChiCTR-IOR-17012905).
Inclusion and exclusion criteria
Inclusion criteria: 1) Achalasia patients undergoing peroral endoscopic myotomy; 2) American Society of Anesthesiologists (ASA) physical status I-II, 18-75 years of age. Exclusion criteria: 1) Preoperative high temperature, increasing white blood cell count (such as recent fever, infection); 2) End-stage tumor with multiple metastases or combined with other tumors; 3) Allergy to dezocine or parecoxib.
ERAS pathway vs. conventional care
Patients were enrolled consecutively and randomized to the conventional or ERAS group. The protocols of the two groups are displayed in Table I.
Table I
Comparison of the protocol of the two study groups
ERAS protocol
Briefly, for the ERAS group, the day before the surgery, the patients received elaborate preoperative information including the program of anesthesia and surgery, and were encouraged to resume oral feeding and mobilize early after surgery. The patients could take a low fiber and low residue diet until 6 h before surgery and water until 2 h before surgery. During the operation, the fluid rate was maintained at 3–5 ml/kg·h to avoid any fluid overload. The room temperature was maintained at 21–23°C, and relative humidity was maintained at 55–60%. Patients were warmed by the heater after entering the room. The liquids were pre-warmed in a 42°C incubator before use. The tympanic membrane temperature was monitored during the operation and the tympanic membrane temperature was maintained at 36–37°C. After surgery, patients were treated with parecoxib sodium 40 mg q12 h (8:00 am, 8:00 pm). Postoperative pain was measured using the Visual Analogue Scale (VAS) and the use of additional analgesics was recorded.
Conventional care protocol
Briefly, before the surgery, the patients of the conventional group received brief preoperative information. The patients avoided oral food intake 8 h before surgery and avoided water intake 6 h before surgery. During the operation, the fluid rate was maintained at 8–10 ml/kg·h. The room temperature was maintained at 21–23°C, and relative humidity was maintained at 55–60%. Patients did not receive any additional insulation measure. The tympanic membrane temperature was monitored during the operation. After surgery, patients were treated with dezocine (5 mg). Postoperative pain was measured using the Visual Analogue Scale (VAS) and the use of additional analgesics was recorded.
Anesthesia
Before anesthesia, patients of the two group underwent gastroscopy to remove residual food from the esophagus and stomach. Anesthesia was induced with intravenous propofol (2 mg/kg), fentanyl (2 μg/kg), remifentanil (0.2 μg/kg/min) and suxamethonium chloride (1.5 mg/kg). Desflurane (MAC: 0.8–1.0) and remifentanil (0.05 μg/kg/min) were administered for maintenance of anesthesia. Additionally, fentanyl was administered if the operation time was more than an hour. All patients received standardized POEM by a practicing physician. At the end of surgery, all subjects received tropisetron (6 mg).
Outcome measures
The primary endpoint was standard postoperative length of stay (LOS). The standard postoperative LOS was identified that patients were satisfied with the following conditions:
Oral analgesic drug pain control is satisfactory (VAS ≤ 3).
Satisfied with the conditions for resuming taking in liquids after POEM:
Independent activity.
All drainage tubes have been pulled out.
Vital signs are stable, such as heart rate, blood pressure, respiratory rate, body temperature, etc.
Patients were evaluated at 8 am and 4 pm daily after surgery to assess whether the above discharge criteria were met.
The secondary endpoints included the length and costs of hospital stay, QoR-15 score [13], VAS and various functional recovery parameters such as time for resumption of oral feeding, first passage of flatus and walking. The other secondary endpoints included morbidity parameters such as the need for extra analgesics, incidence of postoperative nausea and vomiting (PONV), subcutaneous emphysema, pneumoperitoneum, pneumothorax, pneumomediastinum, infection, and readmissions.
Sample size calculation
Sample size was calculated to detect the standard postoperative LOS, with an α error of 0.05 and a β error of 0.2. The formula Ne = Nc = 2 × (Uα /2 + Uβ)2 × σ2/δ2 was used to calculated the sample size. Σ = [(Se 2 + Sc 2)/2]0.5, δ = Xe – Xc. σ and δ were calculated from our pre-experiment (data not shown). The sample size was calculated at 25 patients per group. Moreover, considering a potential 10–15% dropout or lost to follow-up rate, the number of each group was at least 30. Finally, we planned to enroll 40 patients in each group.
Statistical analysis
Continuous data are presented as means ± SD. Categorical variables are reported as numerical counts and percentages. Statistical analysis was performed with SPSS 17.0 software (SPSS Inc., Chicago, IL, USA). Student’s t test or Fisher’s exact test was used to evaluate significant differences. A p-value < 0.05 was considered statistically significant.
Results
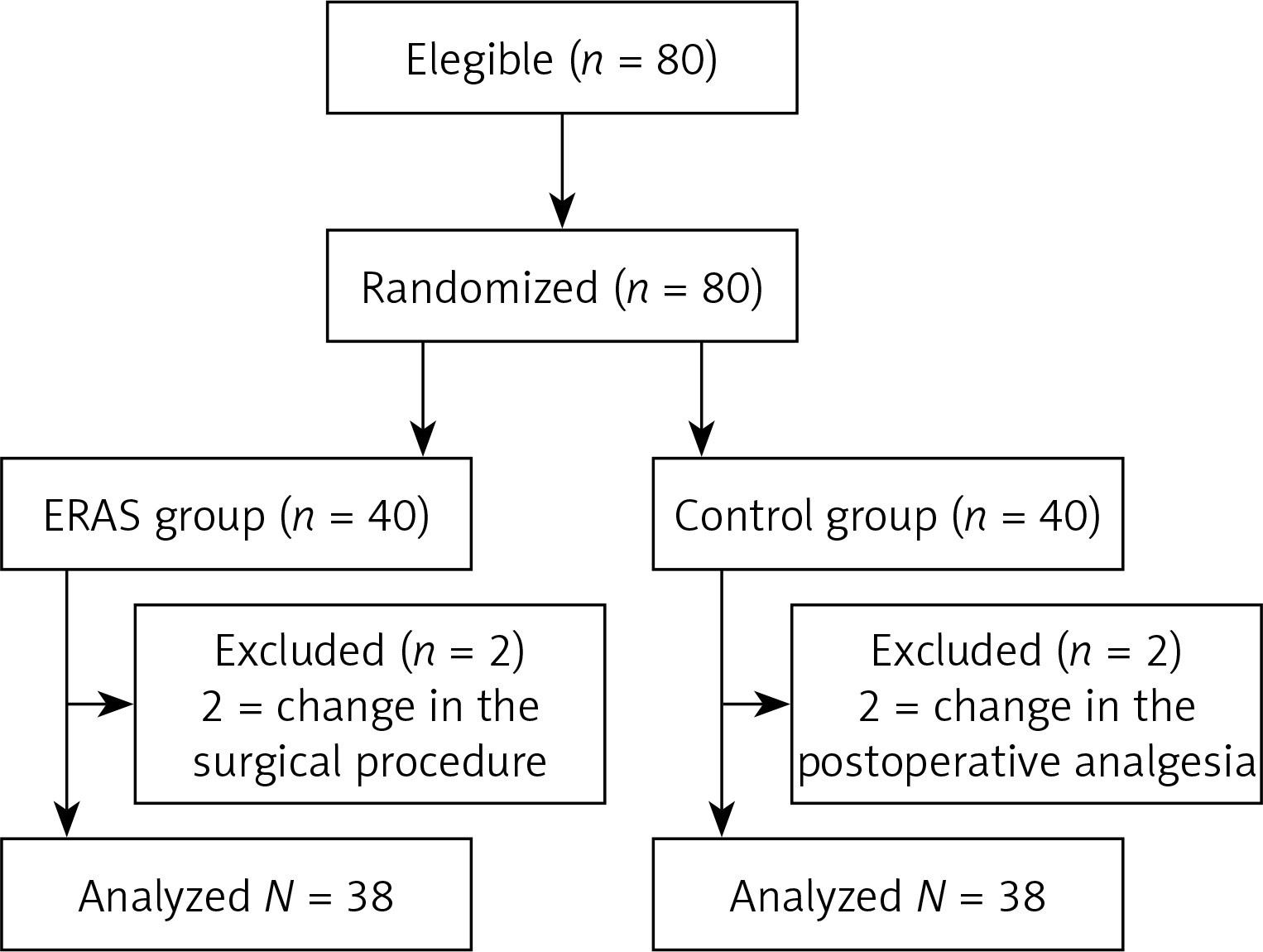
Eighty patients were eligible, and 76 were analyzed (38 in ERAS group, 38 in conventional group). The flowchart of the study can be seen in Figure 1. Table II displays the demographic and clinical characteristics of the two groups. The mean age of the entire population was 38.41 years: 40.21 in the ERAS group and 36.61 in the conventional group. The duration of the operations ranged from 30 to 200 min (mean = 83.95 min) for the ERAS group and 40 to 215 min (mean = 77 min) for the conventional group (p = 0.390). No patients in either group were re-admitted to the hospital during 28 days of follow-up, or required another surgical intervention or a blood transfusion in the two groups.
Table II
Demographic and intra-operative parameters of the 2 groups
Primary outcome
We compared the standard postoperative LOS. The standard postoperative LOS of the ERAS group was significantly shorter than that of the conventional group (40.21 ±8.42 h vs. 48.63 ±10.42 h; p < 0.001) (Table III).
Table III
Primary and secondary outcomes
Secondary outcomes
Length and cost of stay
The patients of the ERAS group (61.90 ±14.73 h) stayed a mean of 6.31 h less than the conventional group (68.21 ±16.61 h), but the difference was not significant (p = 0.084). The costs of stay between the two groups were similar (ERAS group vs. conventional group: ¥26788.76 ±3393.16 vs. ¥26201.51 ±3521.63; p > 0.05) (Table III).
Intraoperative temperature
The changes of intraoperative temperature in the two groups are shown in Figure 2. The temperature of the ERAS group was significantly higher than that of the conventional group from 30 min after surgery to the post-anesthesia care unit (PACU) (p < 0.05). However, there was no significant difference in the frequency of hypothermia between the two groups (Table III).
Figure 2
Intraoperative temperature
Tem_T1 – preoperative temperature, Tem_T2 – temperature at the beginning of surgery, Tem_T3 – temperature at 30 min after starting surgery, Tem_T4 – temperature at the end of surgery, Tem_T5 – temperature in PACU; *p < 0.05, compared with the temperature at the beginning of surgery in the same group; #p < 0.05, compared with the conventional group at the same time.

QoR-15 scores
Table III shows QoR-15 scores for the ERAS and conventional groups. On postoperative day 2, QoR-15 score was significantly higher in the ERAS group than that in the conventional group (139.29 ±2.21 vs. 137.03 ±3.77; p = 0.002). Moreover, the scores improved after surgery in both groups.
Post-operative courses
The ERAS group returned to the oral liquid diet earlier than the conventional group (31.80 ±8.7 h vs. 42.35 ±10.80 h; p < 0.001, Table III). Also the postoperative intestinal exhaust time of ERAS group patients was earlier (18.96 ±8.59 h) than the conventional group (26.35 ±10.26 h; p = 0.001). However, there was no significant difference in the time of mobilization between the two groups (p < 0.05).
Post-operative pain
Post-operative VAS scores among the patients are presented in Figure 3. The VAS scores at 4–24 h after surgery were significantly lower than those at 2 h after surgery in both groups. The VAS scores of the ERAS group were significantly lower than those of the conventional group after the operation (p < 0.05). However, incidences of post-operative VAS more than 3 are documented in Table III, which were similar in the two groups.

Functional recovery parameters
Patients in the ERAS group had a significantly early return of bowel functions in terms of occurrence of first flatus, and earlier resumption of oral feeding (Table III). For the length of resuming mobilization, there was no significant difference.
Post-operative complications
The post-operative complications in the two groups are presented in Table III. There was no significant difference in the incidence of subcutaneous emphysema, pneumoperitoneum, postoperative nausea and vomiting, pain and fever between the ERAS group and conventional group (p > 0.05). Further, there was no re-admissions after 28 days of discharge in the two groups.
Discussion
This was a prospective, randomized pilot study aiming to compare the modified ERAS protocol with the standard care in patients undergoing POEM. We have observed several benefits associated with the use of the ERAS protocol including significantly shorter time of standard postoperative LOS, as well as faster recovery of gastrointestinal function and improved postoperative satisfaction of patients.
The traditional preoperative fasting time is 8–10 h, aimed at avoiding reflux and vomiting during anesthesia. For achalasia patients undergoing POEM, fasting for a longer time is widely accepted. Several studies have adopted a clear liquid diet for more than 48 h prior to the procedure, and nil per os (NPO) after midnight on the day of the procedure [14, 15]. In our study, we allowed patients to take a low fiber and low residue diet until 6 h before surgery and water until 2 h before surgery. For shorter fasting, we did not observe anesthetic complications, and the ERAS group recovered faster. Therefore, shortening preoperative fasting is safe and feasible, but the effects of this measure need further study.
The ERAS protocol produced significant results in earlier readiness for hospital discharge and resumption of oral intake. Optimized perioperative management together with modified analgesic therapy maintained body homeostasis better. Perioperative body temperature drop would increase cardiac adverse events, intraoperative hemorrhage, postoperative wound infection, anesthetic recovery time, postoperative gastrointestinal recovery time, LOS and hospital costs [16, 17]. The physical warming measure in this study effectively maintained intraoperative normothermia, and body temperature fluctuation was less than 0.1°C. In our study, we also demonstrated that controlled perioperative fluid administration is suitable for POEM, which could avoid the adverse effects of excessive intravascular volume, such as increasing demands on cardiac function and delaying the resumption of gastrointestinal function [18].
For postoperative analgesia, dezocine is an effective painkiller, but may cause greater respiratory depression and may cause opioid withdrawal syndrome in patients already using other opioids [19]. Cyclooxygenase-2 inhibitors (COX-2) are effective to reduce postoperative pain and improve patients’ postoperative satisfaction, without the side effects associated with conventional non-selective NSAIDs that result in COX-1 inhibition [20–24]. We found that parecoxib sodium is equivalent to or better than dezocine for the postoperative analgesic effect.
QoR-15 has been widely used to assess postoperative recovery where higher scores correlate with improved recovery and well-being [25, 26]. Through QoR-15, we found that the ERAS protocol promotes postoperative recovery. Moreover, the ERAS protocol did not lead to an increase in local or systemic complications, thus confirming the safety of this protocol.
This study has several limitations. First, the study subjects were enrolled from one hospital, and the number of patients was small. Second, only patients of Asian ethnicity were included, and the findings may not be applicable to other ethnic groups. Third, for EA patients, shortening preoperative fasting time could have consequences for food residue in the esophagus and stomach, but we did not record the time needed to clear residual food. Fourth, a longer duration of follow-up will be needed to evaluate whether the ERAS protocol could affect the long term efficacy of POEM.