






Ostial calcified lesions still constitute a challenge in invasive cardiology. The risk for restenosis is relatively high, especially when more than one layer of struts is implanted with a suboptimal result. Ostial in-stent restenosis (ISR) within an underexpanded stent could be a challenge especially if non-compliance (NC) or ultra-high pressure balloons are ineffective. Although intravascular lithotripsy (IVL) is not recommended in in-stent lesions, the off-label usage of IVL could be the only chance to improve the clinical outcome [1]. This technique uses a balloon-mounted ultrasound source leading to emission of sonic pressure waves propagating through the fluid and delivered to the coronary artery wall. It results in the fragmentation of both superficial and deep calcium deposits, allowing better balloon expansion. Intravascular imaging including optical coherence tomography (OCT) may deliver extra information about the pathomechanism of restenosis and the most effective treatment. Performance of percutaneous angioplasty (PCI) under OCT guidance has an established scientific position in ostial lesions and recurrent restenosis [2].
The criteria for a comprehensive approach by combining IVL with OCT guidance for the massively calcified recurrent restenosis of two layers of struts in ostial right coronary artery (RCA) were met by a 71-year-old woman with arterial hypertension, hyperlipidemia, diabetes, and history of myocardial infarction, treated in different catheterization laboratories with multiple PCI of ostial RCA (PCI with Promus stent 3.5 × 20 mm implantation – 09.2018, plain old balloon angioplasty (POBA) – 02.2019, PCI with Xience stent 3.0 × 18 mm implantation – 02.2020, paclitaxel-eluting balloon angioplasty – 08.2020). Due to symptoms of unstable angina with critical restenosis in RCA ostium covered by 2 layers of stents (Figure 1 A), the patient was qualified for IVL of ISR of RCA under OCT guidance. After initial predilatation with the NC balloon (2.5 × 15 mm) OCT assessment was done. The multilevel depths of calcium that overgrew the stent struts were visualized with modeling of the uncovered stent struts (Figure 1 B).
Figure 1
A – Critical restenosis under two layers of stents in RCA. B – OCT assessment after first NC balloon 2.5 × 15 mm inflation. C – Final angio after 4.5 × 20 mm paclitaxel-eluting balloon delivery. D – Final OCT assessment
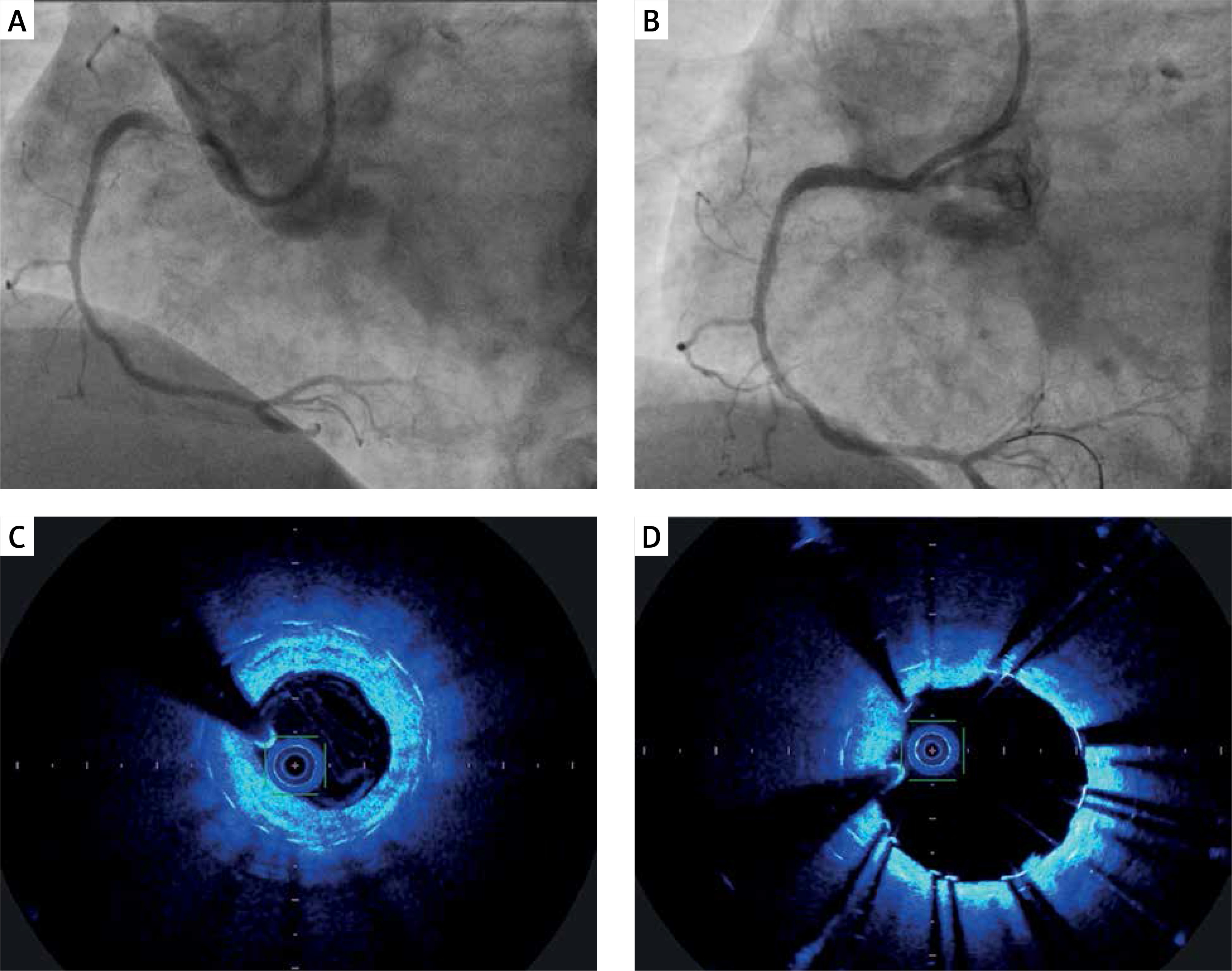
Despite the high pressure (35 atm) inflation of 3.5 × 20 mm ultra-high pressure balloon (OPN), full expansion was not achieved. The procedure was continued using a 4.0 × 12 mm IVL balloon (Shockwave Medical) which, after completing 80 cycles, allowed for visibly better expansion (45%) of the balloon at 6 atmospheres. The effect was optimized by inflation of 4.5 × 15 mm and 5.0 × 15 mm NC balloons and, finally, a paclitaxel-eluting balloon (4.5 × 20 mm) was delivered for 90 s (Figure 1 C). The final OCT visualized correct horizontal position of stent struts with MSA 4.35 mm2 (Figure 1 D) and an acceptable angiographic result. In the opinion of the authors the reason for the difficult-to-expand lesion were two relatively small and primary underexpanded second generation stents implanted in the non-optimally prepared, massively calcified ostial RCA lesion.
Re-stenting an ISR lesion, old underexpanded stents, the amount of neointimal, peri-stent calcium, and multiple, old stent strut layers were found to be the most important determinants of new stent underexpansion, which is then associated with adverse long-term outcomes [2].
Rotational atherectomy, ultra-high pressure balloons, scoring, and cutting balloons or IVL are possible tools in the calcified lesion. Underexpanded stents implanted in heavily calcified segments limit the usefulness of the majority of them. There is still a lack of trials with IVL in ISR; however, sometimes lithotripsy offers an alternative method of treatment. The OCT image provides extra information about malapposed or underexpanded stents with determination of calcium deposits, which could affect stent struts and be the reason for recurrent restenosis. A hybrid approach of preliminary IVL with subsequent NC or ultra-high pressure balloon and final drug-eluting balloon expansion may be the only effective solution to achieve the desired result in persistently recurrent ISR.