





Dear Editor,
This letter introduces a promising perioperative pain management stra-tegy using epidural analgesia with opioids alone, without local anaesthe-tics, for upper extremity surgery in a patient with motor and sensory deficits of the arms and fingers due to chronic inflammatory demyelinating polyneuropathy (CIDP).
This case concerns a 51-year-old man with CIDP (written informed consent for publication was obtained from the patient). Approximately 3 years ago, he experienced sensory disturbances in both lower limbs, mainly in bilateral plantar areas. He was treated with steroid pulse therapy, intravenous administration of immunoglobulin, and plasmapheresis repeatedly. However, his neurological symptoms repeatedly improved and worsened. Recently, he had palsy, gait disturbance in both lower limbs, and sensory disturbance in the plantar region due to the sensory ataxic neuropathy caused by CIDP. The left upper extremity had numbness, hypaesthesia, muscle weakness and difficulty of movement distally from the elbow including his left-side fingers. The right upper extre-mity had numbness distal to the wrist; however, he could still manage to move the right-hand fingers. Thus, he managed to use only his right hand at work and walked with the right hand on crutches.
He suffered a fall at home and had a left proximal humerus fracture (Figure 1). Upon examination, a humeral head replacement was indicated. This procedure is associated with very severe postoperative pain, and general anaesthesia with brachial plexus block is generally the first choice. However, it was unclear whether a brachial plexus block with local anaesthetic was appropriate for our patient as he had pre-existing difficulty in moving his left upper arm and fingers and paraesthesia in his left hand due to CIDP. Therefore, alternative postope-rative pain management strategies were considered, without worsening the numbness and difficulty of movement in the upper arm and fingers. The anaesthesiologist determined that epidural analgesia with opioids alone, without local anaesthetics, was the most suitable for postoperative pain management in this case. Although morphine and fentanyl are the opioids available for neuraxial analgesia in Japan, morphine was chosen to be administered using an epidural catheter. This was because hydro-philic morphine is slowly absorbed by the tissues, can diffuse into the cere-brospinal fluid (CSF), and exerts its analgesic effect in a wider dermatome region in a headward direction on the CSF circulating flow, whereas lipophilic fentanyl is quickly absorbed by the tissues and transferred to the body circulation, resulting in a short duration of action [1, 2]. Thus, it was expected that morphine’s analgesic effect would extend to the brachial plexus region with the epidural cathe-ter inserted at the level of the upper thoracic spine. The intraoperative anal-gesia was planned to be mana-ged primarily using remifentanil because of the slower onset of neuraxial morphine. Remimazolam was selected as the general anaesthetic to confirm that a good analgesia was achieved successfully without changes in neurological findings, such as sensation or difficulty moving the left arm and fingers immediately after surgery. While a previous study reported that rocuronium can be used and antagonized by sugammadex without any problem in patients with CIDP [3], no muscle relaxants were planned for anaesthetic management in our patient, including the tracheal intubation procedure, since muscle relaxation was not essential for the humeral head replacement.
FIGURE 1
Radiograph representing the findings of the left proximal humerus fracture. A complicated fracture with displaced bone fragment at the proximal portion of the left humerus was observed; therefore, a humeral head replacement was indicated

An epidural catheter was inserted 5 cm into the epidural space from the Th2/3 level before general anaesthesia induction. No local anaesthetic test dose was administered. While the patient was preoxygenated, 2 mg of morphine and 5 mL of saline were administered using an epidural cathe-ter. After attaching the bispectral index (BIS) monitor to the patient, a bolus dose of 8 mg of remimazolam was administered to obtain sleep, and continuous administration of remifentanil (0.3 μg kg–1 min–1) and remimazolam (1 mg kg–1 h–1) was initiated. After intubation, surgery was performed in the beach chair position, 55 min after the administration of 2 mg of morphine. Remimazolam was administered continuously at 1 mg kg–1 h–1 until the end of surgery, consulting BIS values as a reference, while remifentanil was adjusted within 0.25–0.3 μg kg–1 min–1. The duration of surgery was 118 min. At the end of the surgery, remimazolam and remifentanil were reduced to 0.5 mg kg–1 h–1 and 0.1 μg kg–1 min–1, respectively, and were stopped after postoperative radiographs were confirmed (Figure 2). After administration of 0.5 mg of flumazenil, the patient was quickly awakened and extubated. The time from morphine administration to extubation was 200 min. Postoperatively, the patient’s left upper extremity was fixed with a triangular bandage. Moreover, it was noted that there was no pain, no change in subjective symptoms of sensation in his left upper extremity, and that he was able to move his left fingers. After confirming the stability of the patient’s arousal and respiratory status, continuous administration of morphine was set at 4 mL h–1 in a balloon system filled with 8 mg of morphine and 300 mL of saline for 3 days; the patient was admitted to the orthopaedic ward. Postoperative pain management was very good with a visual analogue scale pain score of 0 at rest and 1–2 with body movement on the night of surgery, indicating a very high level of patient satisfaction. The patient had not developed any nausea or vomiting in the perioperative period. There was no increase in pain after the conti-nuous administration of morphine via the epidural catheter was completed on the evening of the third postoperative day (POD), and the epidural catheter was removed on the fourth POD. The patient was discharged 21 days after surgery with no worsening of neurological symptoms due to CIDP.
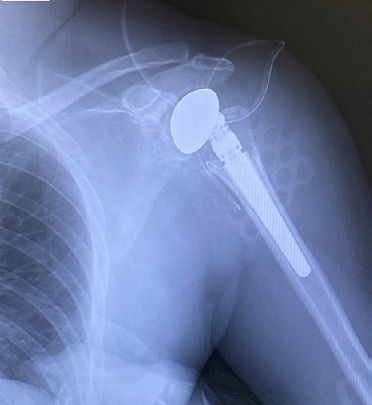
FIGURE 2
Postoperative radiograph after left humeral head replacement. Epidural anaesthesia containing only morphine provided good postoperative pain control with a high level of satisfaction in our patient
CIDP is a rare, progressive, and relapsing neurological disorder which causes peripheral neuropathy, lasting more than two months [4]. CIDP occurs at any age [5], has an incidence of 0.8–8.9 per 100,000 [6], and is more common in males than females [7]. CIDP is thought to be mediated by the auto-immune system through inflammation of nerve roots and peri-pheral nerves and destruction of the myelin sheath of the nerve fibres [8]. As a result, CIDP presents predominantly as slow progression of both proximal and distal muscle weakness, often accompanied by sensory deficits [9].
Limited literature is available on anaesthesia management in patients with CIDP, with no consensus on a standardized anaesthesia mana-ge-ment approach for patients with CIDP. A previous case report described a com-bination of transversus abdominis plane block and rectus sheath block with 0.25% levobupivacaine with total intravenous anaesthesia using propofol, remifentanil, and ketamine without a muscular relaxant for a laparoscopic Hartmann’s operation. The postope-rative analgesia was performed by intravenous patient-controlled analgesia using fentanyl (12.5 µg h–1) with no reported worsening of neurologic symptoms due to CIDP [10]. However, the major challenge in our current case was to provide good perioperative anaesthetic management without a potential impact on neurologic symptoms in the extremities due to CIDP. In another previous report, lumbar anaesthesia was performed using bupivacaine (7.5 mg) for surgery of a femoral neck fracture. The patient was discharged 3 days after surgery without any worsening of neurological symptoms of CIDP [6]. Another report described a case of lumbar and epidural anaesthesia with saphenous and popliteal sciatic nerve blocks for ankle surgery. In this patient, CIDP symptoms transiently worsened on the fourth postoperative day, but the course was considered to be related to perioperative stress, and neurological findings reportedly improved four months later [11].
In our case, satisfactory postope-rative analgesia for humeral head replacement was performed using epidural anaesthesia containing only morphine in a patient with CIDP who had neurologic symptoms in the upper and lower limbs. Considering the onset time of effect, a single-shot bolus of fentanyl using an epidural catheter might speed up the onset time of the analgesic effect, since epidural fentanyl onset is faster than that of epidural morphine. This is due to their respective lipophilic and hydrophilic natures [12, 13]. While continuous administration of morphine was set at 4 mL h–1 in a balloon system in the current case, it was merely because the equipment used at our hospital was a 4 mL h–1 balloon system and the administration rate could be set by the institution.
The diffusion of the hydrophilic morphine to the intrathecal space contri-buted to the effectiveness of the epidural analgesia [1, 2]. Nausea and pruritus have been reported in approximately 20–30% and 20–40% of patients receiving epidural morphine analgesia, respectively [14–16]. One side effect re-quiring attention concerning its hydro-philic property is the possibility of respiratory depression related to epidural analgesia with morphine. The frequency of the respiratory rate falling below 10 breaths per minute was reportedly 0.07% [14], and naloxone administration was necessary in 0.2% of cases of respiratory depression [15]. Thus, the respiratory depression associated with epidural analgesia with morphine is infrequent, and the usual forms of postoperative management, such as SpO2 monitoring, blood pressure measurement, and electrocardiography, are considered sufficient, but such monitoring should be continued at least for the first 24 hours [17].
According to a meta-analysis comparing the efficacy of postoperative pain management among three groups – patient-controlled epidural analgesia with local anaesthetic and/or opioids without basal continuous infusion (PCEA), continuous epidural infusion of local anaesthetic and/or opioids (CEI), and intravenous patient-controlled analgesia (iv-PCA) with opioids – epidural analgesia with PCEA and CEI is significantly superior to iv-PCA for overall pain, pain at rest, and pain with activity; however, PCEA is inferior to CEI in pain management. In addition, hydrolipid opioid alone was significantly inferior in providing analgesia to local anaesthetic alone or local anaesthetic plus opioid in the PCEA group [16]. This may be attri-buted to the slower onset of a neuraxial hydrolipid opioid, such as morphine. Considering these circumstances, the postoperative pain management strategy to administer morphine continuously using an epidural catheter in our current case seems logical.
This letter indicates that epidural anaesthesia using opioids only is a promising postoperative pain mana-gement strategy for both upper and lower extremity surgery in patients with neurological complications. This may even be an option for other types of surgery where epidural anaesthesia may be indicated, such as chest and abdominal surgery.