






Summary
In some patients after acute myocardial infarction (AMI) treated with primary percutaneous intervention and a reduction in left ventricular ejection fraction (LVEF) ≤ 35%, there is a gradual improvement in LVEF. To date, it has not been determined what factors determine the increase. The current study aimed to identify independent predictors of LVEF improvement in patients after AMI treated invasively. Our investigations demonstrated that the presence of severe or moderate mitral regurgitation is the most significant factor contributing to the lack of LVEF improvement following AMI. Moreover, the extent of myocardial damage, as indicated by elevated cTnT values, along with compromised adaptation to hypoxia in patients with diabetes, are identified as independent factors associated with reduced chances of an increase in LVEF.
Introduction
Left ventricular ejection fraction (LVEF) remains the most important determinant of morbidity and mortality after an episode of acute coronary syndrome (ACS) [1, 2]. Despite the effectiveness of reperfusion therapy achieved by the primary percutaneous coronary intervention (PCI) and efficient pharmacotherapy, up to 60% of patients do not improve LVEF [3–5]. A decline in LVEF below 35% after ACS is associated with a worse prognosis. In the IRIS trial, 1 in 5 patients died within 3 years [6]. However, Chew et al. showed that a stronger predictor of post-myocardial infarction mortality, than a decline in LVEF below 35%, was the lack of an increase in LVEF after causal treatment [7]. To some extent, the improvement of LVEF has been explained by the mechanisms of myocardial stunning and hibernation [8, 9]. Various factors have been identified as independent predictors of LVEF improvement, e.g., anterior location of acute myocardial infarction (AMI), single-vessel coronary heart disease, Killip class I–II, lower peak troponin I level, and male gender [4, 5, 10]. Despite recent advances, the clinical practice currently lacks a reliable algorithm to accurately predict the improvement of LVEF after ACS. This is especially critical for patients whose LVEF is reduced below 35% and who are considered potential candidates for implantable cardioverter-defibrillator (ICD) placement. Furthermore, there is a dearth of information on the frequency of significant LVEF improvement in the specific subgroup of post-AMI patients with a baseline LVEF below 35%. As of now, this crucial aspect remains undetermined in the existing literature. More research and investigations are required to address these gaps in knowledge and enhance patient care and decision-making processes.
Aim
The primary objective of the present study was to identify and analyze independent predictors associated with lack of LVEF improvement in patients who experienced AMI and received invasive treatment.
Material and methods
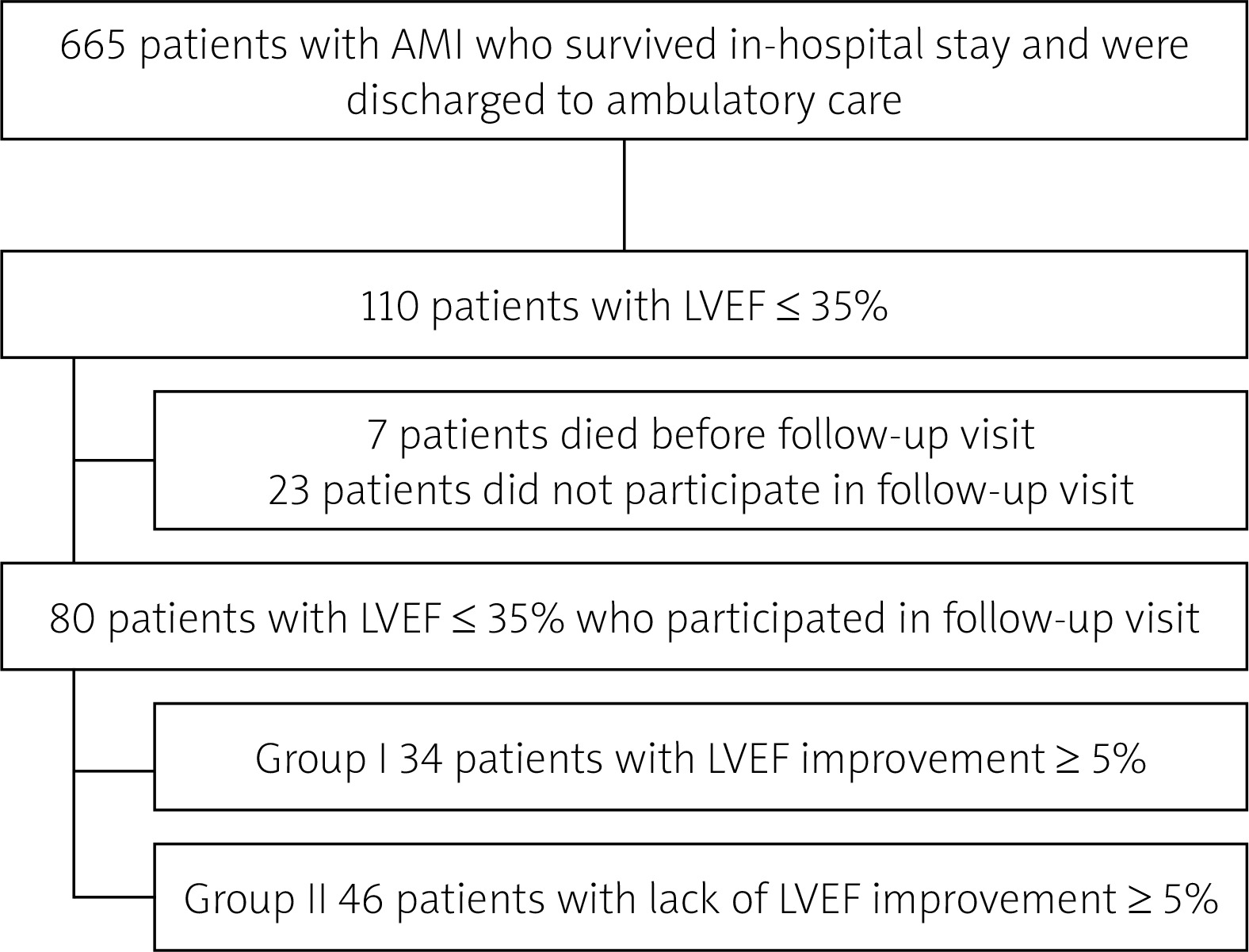
The retrospective observational study encompassed 665 consecutive patients who were admitted with AMI between January 2012 and December 2013. The diagnosis of AMI was established through a combination of typical clinical history, electrocardiographic (ECG) changes observed upon admission, and analysis of enzyme dynamics indicative of myocardial damage. Based on the specific ECG changes, the cases of AMI were further classified as either ST-elevation myocardial infarction (STEMI) or non-ST-elevation myocardial infarction (NSTEMI). Coronary angiography was carried out using the standard approach, with access through either the radial or femoral artery. The decision to proceed with PCI in the infarct-related artery (IRA) was left to the discretion of the experienced interventional cardiologist conducting the study. The cardiologist visually assessed the angiographic images and made an informed judgment on whether PCI was warranted in the specific case. The severity of coronary artery disease was assessed based on the presence of significant or critical stenoses in the coronary vessels. The patients were categorized into three groups: those with single-vessel coronary artery disease, two-vessel coronary artery disease, or three-vessel coronary artery disease depending on the number of affected coronary vessels. Furthermore, the flow in epicardial arteries was evaluated, and the TIMI (Thrombolysis in Myocardial Infarction) scale was utilized for this purpose [11]. The TIMI scale is a widely accepted tool for assessing coronary artery flow and provides valuable information about the perfusion status of the myocardium after a myocardial infarction.
In addition, the study also included the analysis of various blood parameters. These parameters encompassed a complete blood count, electrolyte levels, creatinine levels, cardiac troponin T (cTnT), cardiac fraction of creatine kinase (CK-MB), alanine and aspartate transaminase activity, fasting blood glucose, glycated hemoglobin (HbA1c) and lipogram. By evaluating these blood parameters, the researchers aimed to gain further insights into the patients’ overall health status and assess any potential correlations with LVEF improvement observed during the 6-month follow-up after AMI.
All patients who participated in the study underwent transthoracic echocardiography (TTE) before hospital discharge. From the initial cohort, a subgroup of 110 patients with LVEF of 35% or lower was selected for more in-depth analysis.
Subsequently, patients who passed away during their hospitalization and those who did not attend the scheduled follow-up visit after 6 months were excluded from the analysis. After this exclusion, the final sample size for further investigation comprised 80 patients. These remaining patients were subjected to detailed examination and analysis to identify potential predictors and factors associated with LVEF improvement over the 6-month follow-up (Figure 1). In the study, an increase in LVEF was determined by an absolute rise of ≥ 5% on TTE performed during the follow-up visit, as compared to the initial assessment conducted at discharge or the day before discharge (pre-discharge study). Patients who met this criterion were categorized into Group I, consisting of 34 individuals. On the other hand, Group II comprised patients who did not exhibit an increase in LVEF of ≥ 5% during the follow-up period and consisted of 46 individuals.
Figure 1
Selection of patients for the study group
AMI – acute myocardial infarction, LVEF – left ventricular ejection fraction.
Transthoracic echocardiography
TTE examinations were performed by an experienced echocardiographer using a General Electric Vivid 7 and 9 (2.5 MHz transducer). Wall thickness and dimensions of the left ventricle in diastole (left ventricular end-diastolic dimension) and systole (left ventricular end-systolic dimension) were assessed in 2D presentations from the parasternal long-axis view. Left ventricular volumes and LVEF were calculated using the biplane Simpson method in the apical four-chamber and two-chamber views. The degree of mitral regurgitation was assessed using qualitative (the extent of the regurgitant wave stream using the color Doppler technique), semiquantitative (the width of the vena contracta), and quantitative (the effective regurgitant area) parameters. On this basis, mitral regurgitation was classified as minor, moderate, or severe.
Follow-up visit
The follow-up visit was scheduled in an outpatient setting, precisely 6 months after the patients’ discharge from the hospital. During this visit, all patients underwent a comprehensive assessment, including a thorough subjective and physical examination. Additionally, basic laboratory parameters were determined to gather relevant health-related data. As part of the evaluation, TTE was performed to analyze the changes in LVEF and assess the patients’ cardiac function and recovery progress after AMI.
Ethics
In-hospital management was in accordance with current medical knowledge and the European Society of Cardiology guidelines. All patients gave informed consent to hospitalization, invasive treatment, and usage of clinical data for research purposes. Information about deaths was obtained from telephone interviews with the families of the deceased. Due to its nature, the study did not require approval from the Local Bioethics Committee.
Statistical analysis
The statistical analysis was performed using the JAMOVI software. To assess the distribution of quantitative variables, the Shapiro-Wilk test was applied. For normally distributed data, mean and standard deviation were used to present the results, while median and interquartile range (IQR) were reported for non-normally distributed data. Qualitative variables were presented as counts and percentages. To compare the values of quantitative variables or the frequencies of qualitative variables between different groups, the t-student test, Mann-Whitney test, or χ2 test were used as appropriate.
Regression analysis was conducted to compare different groups, and variables with a p-value of less than 0.1 in the univariate analysis were considered for inclusion in the multivariate model. A significance level of p < 0.05 was used to determine statistically significant findings.
Results
Characteristics of the studied group
The majority of subjects with LVEF ≤ 35% were male, accounting for 58 individuals (72.5% of the sample). The average age of the participants was 65.1 ±10.2 years. Among the subjects, 27.5% had diabetes mellitus, while 66.3% had hypertension. Atrial fibrillation occurred in 10 (12.5%) patients, mostly presented as paroxysmal (80%). Additionally, more than one-third of the patients were diagnosed with obesity based on a body mass index (BMI) greater than 30 kg/m2. Furthermore, 41 (51.2%) individuals were cigarette smokers. A history of previous AMI was noted in 38 patients, representing 48.1% of the study participants. Additionally, 28 (35.4%) patients had previously undergone PCI. Among the patients included in the study, 42 (52.5%) individuals experienced STEMI during their medical history.
The most prevalent location AMI was the anterior wall, which was identified in 33 patients, accounting for 62% of the cases. Among the AMI cases, the left anterior descending (LAD) artery was the most commonly responsible vessel, accounting for 62.8% of the occurrences. The remaining AMI locations were the lateral and inferior walls, observed in 25% and 13% of the cases, respectively.
The mean LVEF at discharge was measured at 29.2 ±4.89%. This value represents the average LVEF among all the patients included in the study at the time of their hospital discharge.
Improvement of LVEF
In the entire study population, there was a significant increase in LVEF from 29.2% at the time of hospital discharge to 35% during the follow-up period (p < 0.001). Specifically, LVEF improvement was observed in 34 out of 80 patients (43%) who initially had reduced LVEF ≤ 35%. Upon comparing the two groups, the increase in LVEF was statistically significant in Group I (p < 0.001), indicating that patients in this group experienced a notable improvement in LVEF during the follow-up period. However, in Group II, the LVEF at the follow-up was comparable to the assessment made at hospital discharge, suggesting no significant change in LVEF in this group during the same period (Figure 2). Patients in Group I were older than in Group II (mean age difference 4.29 years; p = 0.055). In addition, patients in Group I were less likely to have a history of previous coronary heart disease (CHD) (17.6 vs. 37.8%; p = 0.051) and diabetes (14.3 vs. 37.8%; p = 0.02). There were no significant differences in the incidence of STEMI and NSTEMI (51.4 vs. 48.6%; p = 0.535). In the case of STEMI, there were no differences in the location of myocardial infarction between the two groups. This indicates that the distribution of myocardial infarction locations in patients with STEMI was similar in both groups. Patients in Group I had insignificantly lower maximal values of cTnT of 0.913 (IQR = 2.12) ng/ml vs. 1.8 (IQR = 6.72) ng/ml; p = 0.099. No statistically significant differences were found between the two groups regarding the values of CK-MB of 139 (IQR = 239) ng/ml vs. 131 (IQR = 276) ng/ml; p = 0.921.
Figure 2
Comparison of LVEF at discharge and follow-up visit in Group I and Group II
*Statistically significant difference in LVEF at follow-up visit between Group I and Group II. Group I – patients who demonstrated LVEF improvement ≥ 5% at follow-up visit. Group II – patients without LVEF improvement ≥ 5% at follow-up visit.
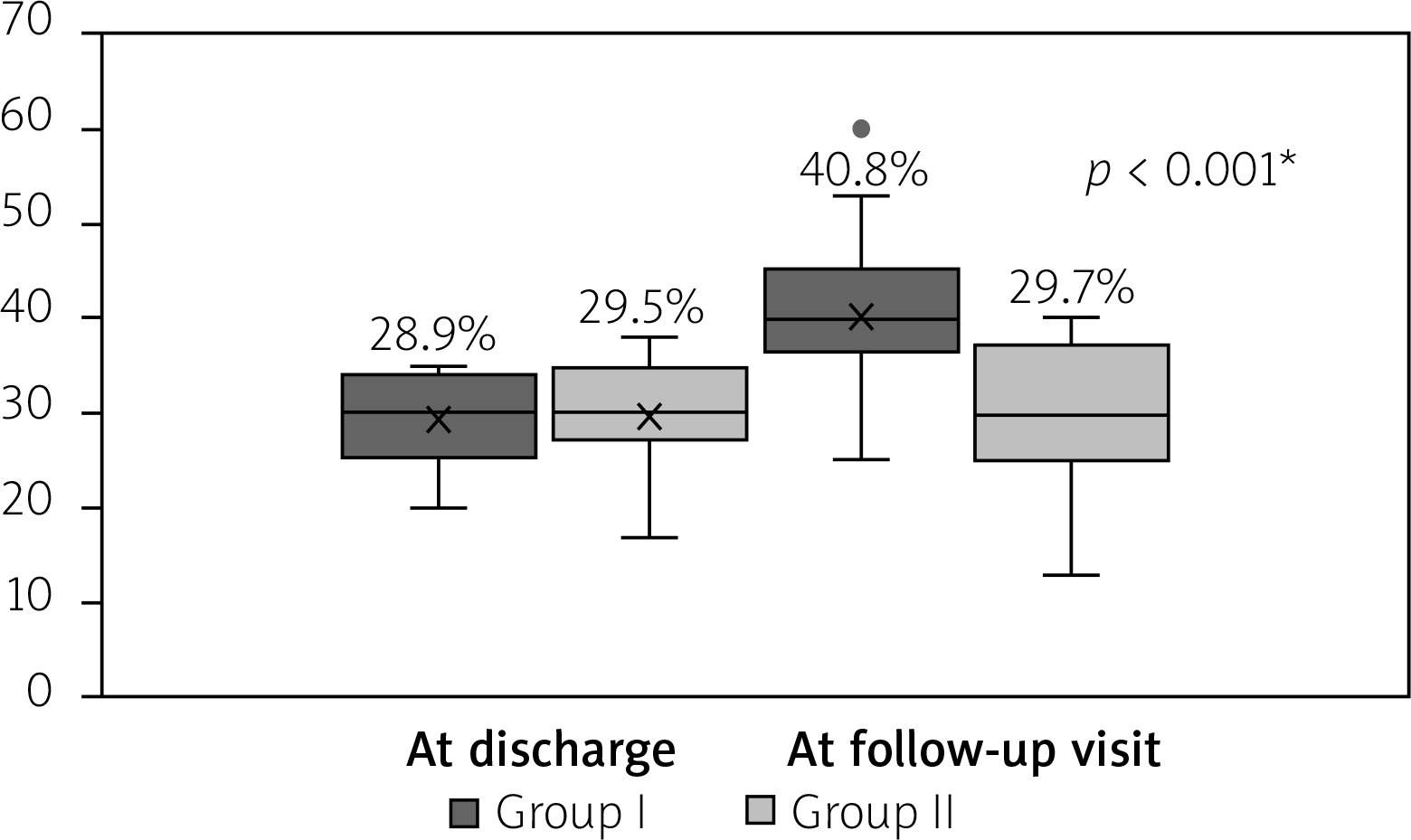
In Group I, the circumflex artery was less often responsible for AMI (0.0 vs. 17.8%; p = 0.009). It was also observed that coronary angiography was less likely to show complete occlusion of IRA or TIMI 0 in Group I compared to Group II (42.9% vs. 65.1%; p = 0.026). There were no differences between Groups I and II in the rate of achieving TIMI 3 flow in the IRA after PCI (85.7% vs. 90.7%; p = 0.394). On TTE performed either at discharge or the day before hospital discharge, patients in Group I exhibited a mean LVEF of 28.9 ±4.67%. On the other hand, in Group II, the mean LVEF measured at the same time was 29.5 ±5.05%. The comparison of LVEF between the two groups showed no statistically significant difference (p = 0.475). This indicates that the initial LVEF values at discharge or the day before were comparable between patients in Group I and Group II (Figure 2). Additionally, the occurrence of moderate and severe mitral regurgitation was significantly less frequent in Group I compared to Group II. Specifically, 22.9% of patients in Group I had moderate to severe mitral regurgitation, while 48.9% of patients in Group II had the same condition. The difference in the frequency of moderate and severe mitral regurgitation between the two groups was statistically significant (p = 0.017). In contrast, there were no significant differences in the number of arrhythmic events and sudden cardiac arrests between Group I and Group II (2.2% vs. 0%; p = 0.375). Analysis of differences in pharmacotherapy showed a trend toward more frequent use of an aldosterone antagonist in Group I (60.0% vs. 38.7%; p = 0.2), but no differences were found regarding the use of β-blockers (100% vs. 97.1%; p = 0.254) and angiotensin-converting-enzyme inhibitors/angiotensin II receptor blockers (91.1% vs. 91.4%; p = 0.96) between both groups. Detailed comparison between the groups is given in Table I.
Table I
Comparison of baseline characteristics between Group I and Group II
| Variable | Group I | Group II | P-value | |
|---|---|---|---|---|
| Gender: | ||||
| Female | n (%) | 9 (25.7) | 13 (28.9) | 0.752 |
| Age [years] | Mean ± SD | 65.2 ±10.2 | 60.9 ±9.4 | 0.055 |
| Hypertension | n (%) | 25 (71.4) | 28 (62.2) | 0.388 |
| Cigarette smoking | n (%) | 19 (54.3) | 22 (48.9) | 0.632 |
| Obesity (BMI > 30 kg/m2) | n (%) | 11 (33.3) | 15 (34.9) | 0.888 |
| Atrial flutter | n (%) | 7 (20) | 3 (6.7) | 0.074 |
| Anterior AMI | n (%) | 13 (37.1) | 20 (44.4) | 0.510 |
| Lateral AMI | n (%) | 6 (17.1) | 7 (15.6) | 0.849 |
| Inferior AMI | n (%) | 3 (8.6) | 4 (8.9) | 0.960 |
| IRA: | ||||
| Left main artery | n (%) | 2 (5.7) | 0 (0) | 0.104 |
| Left descending artery | n (%) | 16 (45.7) | 24 (53.3) | 0.499 |
| Diagonal artery | n (%) | 3 (8.6) | 4 (8.9) | 0.960 |
| Circumflex artery | n (%) | 0 (0) | 8 (17.8) | 0.009* |
| Right coronary artery | n (%) | 10 (28.6) | 7 (15.6) | 0.158 |
| TIMI before PCI: | n (%) | 0.026* | ||
| 0 | 15 (42.9) | 28 (65.1) | ||
| 1 | 6 (17.1) | 5 (11.6) | ||
| 2 | 5 (14.3) | 1 (2.3) | ||
| 3 | 5 (25.7) | 9 (20.9) | ||
| TIMI after PCI: | n (%) | 0.394 | ||
| 0 | 1 (5.7) | 3 (7.0) | ||
| 1 | 0 (0) | 0 (0) | ||
| 2 | 3 (8.6) | 1 (2.3) | ||
| 3 | 27 (85.7) | 39 (90.7) | ||
| Slow-flow | n (%) | 5 (15.6) | 3 (7.1) | 0.244 |
| Total ischemic time [h] | Median (IQR) | 4.0 (10.5) | 4.5 (10.0) | 0.502 |
* p < 0.05, Group I – patients who demonstrated LVEF improvement ≥ 5% at the follow-up visit, Group II – patients without LVEF improvement ≥ 5% at the follow-up visit.
AMI – acute myocardial infarction, BMI – body mass index, CHD – coronary heart disease, CK-MB – cardiac creatine kinase isoenzyme, cTnT – cardiac troponin T, GFR – glomerular filtration rate, IRA – infarct-related artery, non-ST – segment elevation myocardial infarction, PCI – percutaneous coronary intervention, ST – segment elevation myocardial infarction, TIMI – Thrombolysis In Myocardial Infarction.
Logistic regression
The results of univariate logistic regression analysis are presented in Table II. The multivariate model (Table III) revealed several independent factors associated with lack of LVEF improvement after AMI. The factors linked to a reduced probability of LVEF improvement were:
Table II
Univariate regression analysis for baseline variables associated with the improvement of LVEF in post-AMI patients with baseline LVEF ≤ 35%
| Parameter | Odds ratio | Lower 95% CI | Upper 95% CI | P-value |
|---|---|---|---|---|
| Age | 1.0467 | 0.9984 | 1.097 | 0.058* |
| Gender | 0.852 | 0.315 | 2.30 | 0.753 |
| Obesity | 0.933 | 0.358 | 2.43 | 0.888 |
| Diabetes mellitus | 0.275 | 0.0895 | 0.843 | 0.024** |
| Hypertension | 1.518 | 0.587 | 3.92 | 0.389 |
| No history of CHD | 1.733 | 0.705 | 4.26 | 0.230 |
| Chronic kidney disease with GFR < 30 ml/min/1.73 m2 | 1.294 | 0.0781 | 21.45 | 0.857 |
| STEMI | 0.756 | 0.311 | 1.83 | 0.535 |
| NSTEMI | 1.324 | 0.546 | 3.21 | 0.535 |
| Anterior AMI | 0.739 | 0.299 | 1.82 | 0.511 |
| Inferior AMI | 0.961 | 0.201 | 4.6 | 0.960 |
| Lateral AMI | 1.123 | 0.341 | 3.7 | 0.849 |
| IRA – left descending coronary artery | 0.911 | 0.368 | 2.25 | 0.840 |
| IRA – circumflex artery | 0.375 | 0.093 | 1.51 | 0.167 |
| IRA – right coronary artery | 2.171 | 0.730 | 6.46 | 0.163 |
| cTnT | 0.876 | 0.760 | 1.01 | 0.068* |
| CK-MB | 0.999 | 0.996 | 1.0 | 0.367 |
| Slow-flow phenomenon | 2.407 | 0.530 | 10.93 | 0.255 |
| Mild mitral regurgitation | 1.825 | 0.747 | 4.46 | 0.187 |
| Moderate to severe mitral regurgitation | 0.310 | 0.116 | 0.827 | 0.019** |
| Total ischemic time | 0.972 | 0.906 | 1.04 | 0.44 |
| TIMI 0 before PCI | 0.541 | 0.209 | 1.4 | 0.204 |
| TIMI 1 before PCI | 2.22 | 0.568 | 8.68 | 0.252 |
| TIMI 2 before PCI | 6.71e+7 | 0.000 | inf | 0.992 |
| TIMI 3 before PCI | 0.684 | 0.204 | 2.29 | 0.538 |
Table III
Multivariate regression analysis to identify the independent predictors of LVEF improvement in post-AMI patients
| Parameter | Odds ratio | Lower 95% CI | Upper 95% CI | P-value |
|---|---|---|---|---|
| Age | 1.073 | 1.012 | 1.139 | 0.07 |
| Diabetes mellitus | 0.217 | 0.058 | 0.813 | 0.023* |
| cTnT | 0.841 | 0.715 | 0.989 | 0.037* |
| Moderate to severe mitral regurgitation | 0.178 | 0.053 | 0.597 | 0.005* |
Higher levels of cTnT: Patients demonstrating higher cTnT levels exhibited a reduced probability of undergoing improvements in LVEF during the follow-up interval. The chance of LVEF improvement decreased with increased cTnT concentration (OR = 0.841 for 1 ng/ml increase in cTnT, 95% CI: 0.715–0.989; p = 0.037).
Presence of diabetes mellitus: Patients diagnosed with diabetes were more likely not to demonstrate improvements in LVEF in comparison to those without diabetes (OR = 0.217, 95% CI: 0.058–0.813, p = 0.023).
Presence of moderate or severe mitral regurgitation: Patients with moderate or severe mitral regurgitation had a significantly lower chance of LVEF improvement (OR = 0.178, 95% CI: 0.053–0.597; p = 0.005).
These findings emphasize the significance of these factors in predicting LVEF recovery and highlight their potential implications for risk assessment and management in patients with reduced LVEF after AMI.
Discussion
The current study provides compelling evidence that the absence of diagnosed diabetes mellitus, moderate or severe mitral regurgitation, and lower cTnT concentration are all independent factors associated with improved LVEF in patients with ejection fraction ≤ 35% following AMI and invasive treatment at a 6-month follow-up. Notably, the findings regarding lower cTnT levels being linked to LVEF improvement align with existing data reported in the literature. This reinforces the consistency and validity of the study’s results with prior research in this field. Kim et al. showed that lower troponin I level in patients with STEMI was a predictor of improved LVEF [4]. In a multicentre observational study, Brooks et al. demonstrated that a lower troponin value was associated with improved LVEF ≥ 35% at 90-day follow-up [12]. Higher troponin I level reflects a larger area of myocardial infarction as measured by cardiac magnetic resonance imaging and indicates irreversible myocardial damage [13]. Several previous studies have proven that the troponin level in the first days after AMI can predict the degree of left ventricular dysfunction in remote observation, and the higher the value, the greater the damage [14–16]. The area of myocardial infarction is also a predictor of reverse left ventricular remodeling associated with a poorer prognosis of post-AMI patients [17].
In our study, multivariate analysis showed that the presence of moderate or severe mitral regurgitation was an independent factor for lack of improved left ventricular systolic function. To our knowledge, no similar association has been described in the available literature. Mitral regurgitation after AMI occurs in 6% to 64% of patients [18, 19], while moderate or severe regurgitation occurs in 6 to 12%, respectively [20]. The incidence of mitral regurgitations is much lower when patients are treated with PCI [21]. Data on the association of mitral regurgitation incidence with AMI location are controversial. Earlier studies showed that mitral regurgitation was more common in patients with inferior wall infarction [22, 23]. In contrast, Fazlinezhad et al. observed a higher incidence of mitral regurgitation in patients with LVEF ≤ 35% and anterolateral wall infarction [24]. Mechanisms leading to mitral regurgitation in post-myocardial infarction patients are multifactorial. Left ventricular dilatation due to ischemic injury impairs leaflet coaptation of a structurally normal mitral valve. Furthermore, papillary muscle displacement as a result of left ventricular remodeling causes leaflet tethering, dilatation and flattening of the mitral annulus [25]. Mitral regurgitation after AMI has unfavorable prognostic significance, leading to left ventricular volume overload and enlargement, which can lead to reverse remodeling and secondary left ventricular enlargement and further exacerbate functional mitral regurgitation [26]. This mechanism may explain the lack of improvement in LVEF in our group of patients.
The use of renin-angiotensin system inhibitors and β-blockers is widely recommended for patients with reduced ejection fraction to reduce mortality, morbidity, and the risk of heart failure hospitalization [27]. These medications have been shown to have beneficial effects on reverse remodeling or at least deceleration of adverse myocardial remodeling in patients with reduced LVEF [28]. Additionally, there is a possibility that these remedies may secondarily reduce significant mitral regurgitation. However, in the present study, although patients who improved their LVEF were more often prescribed aldosterone receptor antagonists, the difference was not statistically significant. This suggests that while aldosterone receptor antagonists might play a role in LVEF improvement, further research and larger sample sizes may be needed to establish a statistically significant association.
The presence of diabetes mellitus was identified as a predictor of reduced chances of LVEF improvement in the present study. This finding is consistent with previous research indicating that diabetes is more frequently diagnosed in post-AMI patients with reduced LVEF (≤ 35%) compared to those without diabetes (42.5% vs. 32.2%, respectively; p = 0.81) [12]. Post-myocardial infarction patients with concomitant diabetes also had a higher risk of cardiac events, heart failure, and death [29]. However, to our knowledge, the current study is the first which proved the association of the absence of diabetes with improvement in systolic fraction in patients after AMI. Ohashi et al. also observed a less frequent occurrence of diabetes in patients with improved LVEF, but the difference was not statistically significant (43.5% vs. 55.6%; p = 0.15) [30]. Diabetes disorganizes the metabolism of cardiac muscle cells. One of the main abnormalities is the inability to metabolize pyruvate, which in case of energy deficit, causes persistent damage to cardiomyocytes. Another aberration is elevated levels of free fatty acids and their increased consumption by cardiomyocytes, resulting in hypertrophy, ischemia, decreased systolic function, and increased risk of arrhythmias [31]. Diabetes is an independent predictor of left ventricular remodeling by increasing left ventricular mass and myocardial wall stiffness, which decreases systolic function. In addition, it accelerates aortic stiffness and increases afterload [32]. All these pathophysiological abnormalities, which also translate to morphological changes of the left ventricle, may contribute to a lower propensity for LVEF improvement despite reperfusion of the infarcted myocardium. The current study’s results reinforce the significance of diabetes as a risk factor for reduced LVEF and suggest that the presence of diabetes may impede the improvement of LVEF in patients after AMI. Consequently, optimizing the management of diabetes in this patient population may be crucial in improving cardiac outcomes and facilitating LVEF recovery.
A major limitation of the study is its retrospective nature and a small number of patients. Furthermore, the interpretation is based on single-center results. Also, a more accurate assessment of ejection fraction is possible with imaging modalities such as magnetic resonance imaging or scintigraphy, whereas only 2D echocardiography was used in this study. Another limitation is the lack of assessing the influence of angiotensin receptor neprilysin inhibitor and sodium-glucose co-transporter 2 inhibitors on LVEF improvement due to enrolling the patients between 2012 and 2013.
Conclusions
The main finding of the study is the identification of factors associated with a lower likelihood of improving LVEF in patients with myocardial infarction treated invasively. These factors include the presence of moderate to severe mitral regurgitation, diabetes, and higher cTnT concentrations. Indeed, the findings of the current study have significant implications for clinical practice. The identification of factors associated with a reduced likelihood of LVEF improvement in patients with initially significantly reduced LVEF (≤ 35%) after AMI can aid in risk stratification and patient management. These patients may be at higher risk of adverse cardiac events and sudden cardiac death. Recognizing this high-risk subgroup is crucial as they could be potential candidates for ICD placements.