

Purpose
Plaque brachytherapy is a common treatment modality for small- to medium-sized uveal melanoma (≤ 10 mm in apical height and ≤ 16 mm in diameter) [1-3]. Since the prospective randomized Collaborative Ocular Melanoma Study (COMS) trial showed that plaque brachytherapy offers equivalent tumor control with better quality of life in comparison to enucleation [2], plaque brachytherapy has become the standard of care [3]. Different types of plaques have been designed, tested, and clinically used by various investigators [1, 4-10]. While ruthenium-106 (106Ru) plaques are preferred in Europe and Asia, iodine-125 (125I) or palladium-103 (103Pd) plaques are more commonly used in North America [10].
Of various types of plaques, COMS plaques have been widely adopted in North America [2, 11]. The standard COMS plaques consist of a gold-alloy backing (trade name Modulay, density of 15.8 g/cm3) and a Silastic insert (density of 1.12 g/cm3) [12, 13]. Modulay backing provides shielding for surrounding normal tissues, and Silastic insert glued inside Modulay backing accommodates seeds in positions designated in the American Association of Physicists in Medicine task group (AAPM TG)-129 report [13]. Seven different COMS plaque sizes with diameters ranging from 10 mm to 22 mm in 2 mm increments are available [13]. The total number of seeds depends on the plaque diameter (5, 8, 13, 13, 21, 24, and 21 seeds for 10-, 12-, 14-, 16-, 18-, 20-, and 22-mm plaques, respectively) [13]. Common types of seeds used for COMS plaques are 125I and 103Pd seeds [12].
In the effort to improve the AAPM TG-43 formalism-based dosimetry, heterogeneous dose calculations for COMS plaques were performed using Monte Carlo (MC) methods [11, 12, 14-18]. Known contributing factors to heterogeneity corrections for COMS plaques include Modulay backing, Silastic insert, and interseed attenuation effects. Magnitudes of contributing factors for central axis points have been studied [17, 18]. From MC simulations using BrachyDose, Thomson et al. investigated dose reductions by the effects of Modulay backing alone, and Modulay backing and Silastic insert for a 125I single seed and a 103Pd single seed in a 20-mm COMS plaque [17]. With Modulay backing alone, central axis dose decreases within a depth of 22.6 mm were up to 11% and 6.3% for a 125I seed (model: Oncura 6711, Oncura, Inc., Princeton, NJ) and a 103Pd seed (model: Theragenics 200, Theragenics Corporation, Buford, GA), respectively [17]. Corresponding central axis dose decreases due to the combined effect of Modulay backing and Silastic insert were 18% and 21% [17]. Interseed effects were < 1.0% and < 0.5% for a 16-mm COMS plaque fully loaded with 125I and 103Pd seeds, respectively [17]. Zhang et al. also investigated central axis dose reductions by the effects of a gold plaque alone, a gold-alloy plaque alone, and interseed effects for 125I (model: IsoAid IAI-125A, IsoAid, LLC., Port Richey, FL) and cesium-131 (131Cs; model: IsoRay Cs-1 Rev2, IsoRay Medical, Inc., Richland, WA) COMS plaques, by performing MC simulations using MCNPX with an assumption of a water equivalent seed carrier [18]. They reported corresponding dose reductions by up to 18%, 13%, and 4% within a depth of 22 mm for a 16-mm 125I COMS plaque, and by up to 18%, 15%, and 2% for a 16-mm 131Cs COMS plaque [18]. Despite this newly discovered information, the previous studies have limitations: 1. The magnitudes of contributing factors for off-axis points were not investigated; 2. A dose reduction by the effect of Silastic insert alone was not considered independently; and 3. The investigation was not made for 10-, 12-, 14-mm, and 18-, 20-, 22-mm COMS plaques with fully loaded seeds. To overcome these limitations, in this work, the sensitivity of individual contributing factors to heterogeneity corrections in dosimetry of ocular brachytherapy using 125I COMS plaques was comprehensively investigated using an MC method.
Material and methods
Central axis and off-axis points for COMS plaques
Central axis and off-axis dose calculation points for the COMS plaques are described in the COMS protocol (COMS manual) [4]. Central axis points include inner sclera (depth of 0 mm), tumor apex (depth of 5 mm), eye center (depth of 11 mm), and opposite retina (depth of 22 mm) (COMS manual). Off-axis points involve optic disc, macula, and lens center (COMS manual). Typically, four parameters are measured in a fundus diagram to determine coordinates of off-axis points: a tumor basal dimension at the center in the direction from optic disc (BD), a distance from the optic disc to tumor margin (DT), a tumor basal dimension at the center in the direction from macula (BM), and a distance from the macula to the tumor margin (MT). Additionally, tumor apex (i.e., apical height) in the central axis is measured on an ultrasound image. Figure 1 in Lee et al. [2] shows a fundus diagram with the four parameters (BD, DT, BM, and MT), and a cross-section diagram of the eye with apical height.

MC simulations for homogeneous and heterogeneous dose calculations
For MC simulations, egs_brachy (version 0.9.1) was employed. The egs_brachy is an EGSnrc code-based open-source MC tool available for various geometry models and brachytherapy seed models. Its validation for a 16-mm COMS plaque was performed by Chamberland et al. [19]. In the egs_brachy, a COMS plaque is modeled at the center of a water phantom (dimension: 30 cm × 30 cm × 30 cm; density: 0.998 g/cm3). To calculate dose distributions around the plaque inside the eye, in this study, a dose scoring region was set to a volume of 2.55 cm x 2.55 cm x 2.55 cm with a voxel size of 0.05 cm x 0.05 cm x 0.05 cm. For heterogeneous dose calculations, material properties of seeds (model: IsoAid IAI-125A) and of the media in COMS plaques (Modulay backing and Silastic insert) were kept the same as in the literature [20, 21]. The MC code used cross-sections from the XCOM database for Rayleigh scattering, bound Compton scattering, photo-electric absorption, and atomic relaxations [22]. Photon cutoff energy was set to 1 keV, and electron transport was not modelled. For a variance reduction technique, the global range reduction method was used with a history-by-history statistical method. Post-processing was not performed. Absorbed dose to water was reported. Using a 2.5 GHz Intel Xeon® processor with 20 parallel processing CPU cores, a computational time for one COMS plaque was about 105 seconds (~28 hours) for 1010 histories with a statistical uncertainty < 0.5%.
Using the egs_brachy, eight MC simulations were performed for a 16-mm diameter COMS plaque loaded with 125I seeds (model: IsoAid IAI-125). The first simulation, named HOMO, was done under TG-43 assumptions with fully loaded seed configurations in a homogeneous water medium and without Modulay backing, Silastic insert, and interseed effects [20]. This was a direct MC simulation with all media set as water, rather than a dose calculation using the AAPM TG-43 formalism. For HOMO, 85 Gy was prescribed to a central axis depth of 5 mm. The next seven simulations, named HETERO#1-#7, were performed with the same seed configurations but with medium-heterogeneity for the following seven scenarios: #1. Modulay backing alone, #2. Silastic insert alone, #3. Interseed effects alone, #4. Modulay backing + Silastic insert, #5. Modulay backing + interseed effects, #6. Silastic insert + interseed effects, and #7. Modulay backing + Silastic insert + interseed effects, with the rest of the media assumed as water. Table 1 summarizes the assumed medium materials for the Modulay backing and Silastic insert with or without interseed effects in each MC simulation. From HOMO and HETERO#1-#7, homogeneous dose (DHOMO) and heterogeneous dose (DHETERO#1-#7) were determined for central axis points from a depth of 0 mm (inner sclera) to 22 mm (opposite retina), and for off-axis points (optic disc, macula, and lens center) as a function of DT (optic disc) or MT (macula and lens) up to 22 mm for various BDs (optic disc) or BMs (macula and lens) < 20 mm in 2-mm intervals. In the same fashion, MC simulations were completed for the other six 125I COMS plaques (10-, 12-, 14-mm, and 18-, 20-, 22-mm diameter), and DHOMO and DHETERO#1-#7 were determined.
Table 1
Monte Carlo (MC) simulations performed in this study
Determination of HCFs for central axis and off-axis points for seven scenarios
From DHOMO and DHETERO#1-#7 for the 16-mm 125I COMS plaque, heterogeneity correction factors (HCFs) for central axis points and off-axis points were determined for each of the seven scenarios. A ratio of central axis DHETERO#1-#7 to central axis DHOMO was taken to derive central axis HCFs from a depth of 0 mm to 22 mm. Similarly, a ratio of optic disc DHETERO#1-#7 to optic disc DHOMO was taken to derive HCFs for the optic disc as a function of DT up to 22 mm for various BDs < 20 mm in 2-mm intervals. HCFs for the macula and lens were also derived as a function of MT up to 22 mm for various BMs < 20 mm in 2-mm intervals. Correspondingly, HCFs for the rest of the 125I COMS plaques (10-14 mm and 18-22 mm) were determined for the seven scenarios.
Results
HCFs for central axis points for seven scenarios: 16-mm COMS plaque
Table 2 presents HCFs for central axis points for the 16-mm 125I COMS plaque (model: IAI-125A) from scenario #1 to scenario #7 in order. The ranges of dose reductions by the effects of Modulay backing alone (#1), Silastic insert alone (#2), and interseed effects alone (#3) were 0.9-11.3%, 9.0-13.8%, and 0.5-1.7%, respectively (Table 2). At a depth ≤ 1 mm, there was a slight dose increase (up to 0.8%) by Modulay backing alone (#1). A dose reduction by Modulay backing alone (#1) was relatively small (≤ 3.0%) at a depth ≤ 5 mm, but continuously increasing with depth up to 11.3% (depth of 22 mm) (Figure 1). On the other hand, a dose reduction by Silastic insert alone (#2) decreased from 13.8% (depth of 0 mm) as depth increased (depth < 5 mm), reaching a constant value (~9.0%) at 5 mm (Figure 1). A dose reduction by interseed effects alone (#3) increased slightly with depth, but was ≤ 1.7% at a depth ≤ 22 mm (Figure 1). Dose reductions by the combined effects of Modulay backing + Silastic insert (#4), Modulay backing + interseed effects (#5), and Silastic insert + interseed effects (#6), ranged from 12.1% to 19.0%, from 0.0% to 11.2%, and from 9.7% to 14.0%, respectively (Table 2). The combined effect of all three components (#7) reduced a dose ranging from 12.0% to 18.6% (Table 2).
Table 2
Central axis heterogeneity correction factors (HCFs) for a 16-mm COMS plaque loaded with 125I seeds (model: IsoAid Advantage IAI-125A) for seven scenarios (#1-#7)
Because of the small interseed effect (≤ 1.7%) at a depth ≤ 22 mm, the primary contributing factors were the Modulay backing and Silastic insert, and their dominancy was depth-dependent (Table 2, Figure 1). At a depth ≤ 5 mm, the Modulay backing effect was small (≤ 3.0%), and hence the Silastic insert was the dominant factor (range, 9.5-13.8%). At a depth > 5 mm, both the Modulay backing and Silastic insert were contributing factors (range, 12.2-19.0%). In this depth range, the Modulay backing effect increased with depth, whereas the Silastic insert effect did not vary with depth (Figure 1).
HCFs for off-axis points for seven scenarios: 16-mm COMS plaque
Optic disc
Figure 2A-G shows HCFs for the optic disc for the 16-mm 125I COMS plaque (model: IAI-125A) from scenario #1 to scenario #7 in order. The ranges of dose reductions by the effects of Modulay backing alone (#1), Silastic insert alone (#2), and interseed effects alone (#3) were 0.0-12.5%, 9.1-15.3%, and 0.3-2.3%, respectively (Figure 2A-C). The effect of Modulay backing alone (#1) was DT- and BD-dependent (Figure 2A). At short DT ≤ 6.2 mm for all BDs except for BD of 13 mm, slight dose enhancement (constant ~0.9%) was observed. At DT ≤ 6.2 mm, the farthest DT, where constant dose enhancement ends, decreased as BD was increasing. At farther DT ≤ 10 mm, a dose reduction increased with increasing DT for all BDs and with increasing BD at the same DT. At DT > 10 mm, a dose reduction reached the maximum and became constant (~11.1%). The effect of Silastic insert alone (#2) had also a dependence on DT and BD, but was greater (up to 15.3%) than that by Modulay backing alone (#1) for the same BD and DT at DT < 10 mm (Figure 2A, B). A dose reduction by Silastic insert alone (#2) decreased, increased (or just increased for BDs of 9-13 mm), reached the maximum, decreased, and reached the minimum as increasing DT. A dose reduction by the effect of interseed effects alone (#3) increased slightly with depth, but was ≤ 2.3% for all BDs at DT ≤ 22 mm (Figure 2C). Dose reductions by the combined effects of Modulay backing + Silastic insert (#4), Modulay backing + interseed effects (#5), and Silastic insert + interseed effects (#6) ranged from 13.0% to 24.4%, from 0.0% to 12.8%, and from 9.5% to 16.0%, respectively (Figure 2D-F). The combined effect of all three components (#7) reduced a dose by 12.8-24.7% (Figure 2G).
Fig. 2
A-F) Heterogeneity correction factors (HCFs) for the optic disc for a 16-mm 125I COMS plaque (model: IsoAid Advantage IAI-125A) from scenario #1 to scenario #6 in order G) Heterogeneity correction factors (HCFs) for the optic disc for a 16-mm 125I COMS plaque (model: IsoAid Advantage IAI-125A) for scenario #7
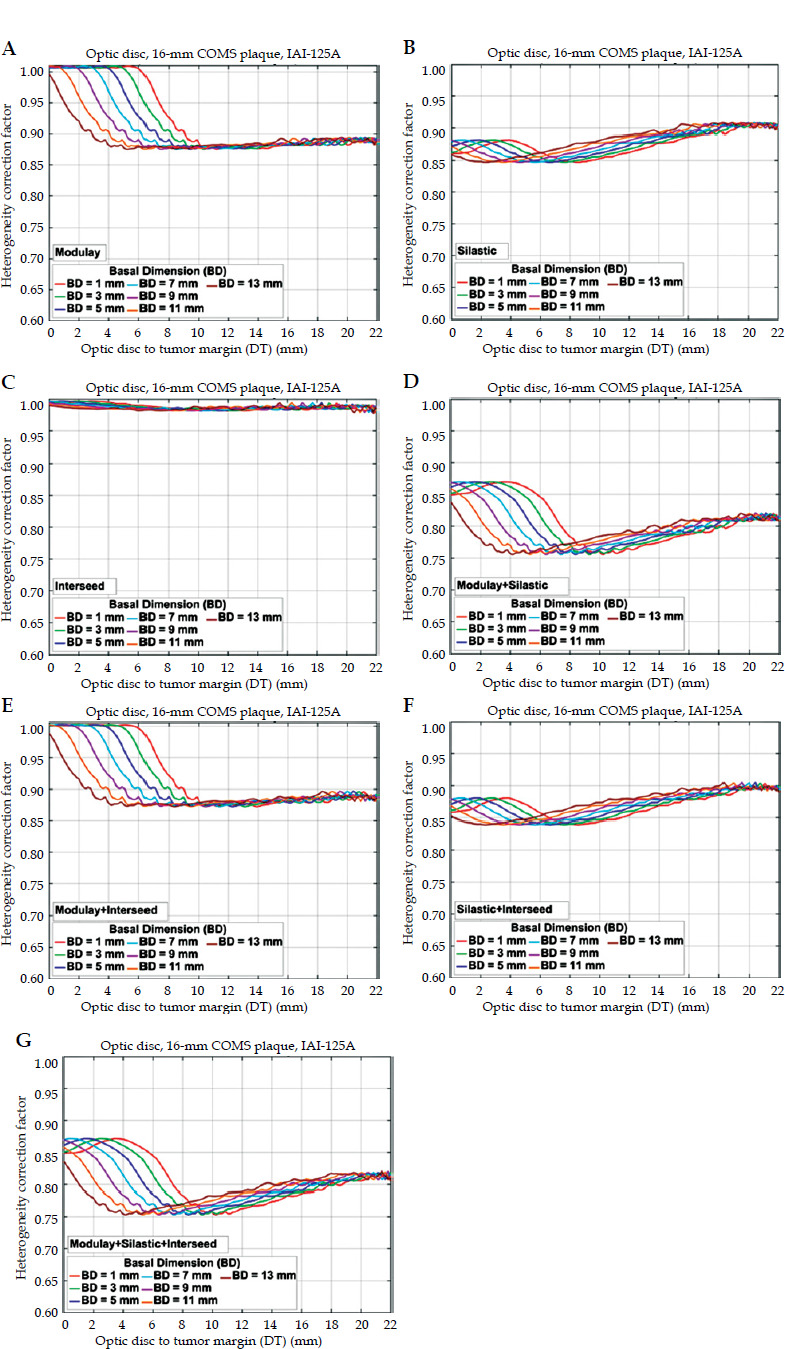
Because of the small interseed effect (≤ 2.3%), the primary contributing factors were the Modulay backing and Silastic insert, and their dominancy was DT- and BD-dependent (Figure 2). At DT ≤ 6.9 mm for BD of 1 mm, at DT ≤ 6.0 mm for BD of 3 mm, at DT ≤ 5.0 mm for BD of 5 mm, at DT ≤ 4.0 mm for BD of 7 mm, at DT ≤ 2.9 mm for BD of 9 mm, at DT ≤ 1.8 mm for BD of 11 mm, and at DT ≤ 0.6 mm for BD of 13 mm, the effect of Modulay backing was ≤ 3%, and therefore, the Silastic insert was the major contributing factor (≥ 11.8%). At farther DT for each BD, both the Modulay backing and Silastic insert were contributing factors (range, 18.3-24.4%).
Macula
Figure 3A-G displays HCFs for the macula for the 16-mm 125I COMS plaque (model: IAI-125A) from scenario #1 to scenario #7 in order. The ranges of dose reductions by the effects of all seven scenarios for the macula were the same as those for the optic disc: 0.0-12.5% (#1), 9.1-15.3% (#2), 0.3-2.3% (#3), 13.0-24.4% (#4), 0.0-12.8% (#5), 9.5-16.0% (#6), and 12.8-24.7% (#7). Dominancy of the contributing factors for the macula was MT- and BM-dependent, and had the same trends but occurred at slightly different MT comparing with that for the optic disc as a function of DT and BD (Figures 2 and 3). For instance, for the macula, the effect of Modulay backing alone (#1) was ≤ 3% at MT ≤ 7.6 mm for BM of 1 mm, at MT ≤ 6.7 mm for BM of 3 mm, at MT ≤ 5.7 mm for BM of 5 mm, at MT ≤ 4.7 mm for BM of 7 mm, at MT ≤ 3.7 mm for BM of 9 mm, at MT ≤ 2.5 mm for BM of 11 mm, and at MT ≤ 1.4 mm for BM of 13 mm (Figure 3).
Fig. 3
A-D) Heterogeneity correction factors (HCFs) for the macula for a 16-mm 125I COMS plaque (model: IsoAid Advantage IAI-125A) from scenario #1 to scenario #4 in order E-G) Heterogeneity correction factors (HCFs) for the macula for a 16-mm 125I COMS plaque (model: IsoAid Advantage IAI-125A) from scenario #5 to scenario #7 in order

Lens
Heterogeneity correction factors for the lens for the 16-mm 125I COMS plaque (model: IAI-125A) are plotted in Figure 4A-G from scenario #1 to scenario #7 in order. Dose reductions by the effects of Modulay backing alone (#1), Silastic insert alone (#2), and interseed effects alone (#3) ranged from 1.9% to 10.2%, from 8.9% to 10.7%, and from 0.5% to 1.8%, respectively (Figure 4A-C). A dose reduction by Modulay backing alone (#1) was almost constant (~10.2%) for all BMs at MT < 7 mm, and at MT ≥ 7 mm, it decreased and reached the minimum (~1.9%) (or reached the minimum and increased) as increasing MT for all BMs (Figure 4A). A dose reduction by Silastic insert alone (#2) did not vary drastically (within 1.8%) for all BMs at MT ≤ 22 mm (Figure 4B). A dose reduction by interseed effects alone (#3) decreased slightly with MT, but was small (≤ 1.8%) for all BMs at MT ≤ 22 mm (Figure 4C). The ranges of dose reductions by the combined effects of Modulay backing + Silastic insert (#4), Modulay backing + interseed effects (#5), and Silastic insert + interseed effects (#6) were 12.0-18.2%, 2.3-10.5%, and 9.8-11.5%, respectively (Figure 4D-F). The range of a dose decrease by all three components (#7) was 12.0-18.2% (Figure 4G).
Fig. 4
A-F) Heterogeneity correction factors (HCFs) for the lens for a 16-mm 125I COMS plaque (model: IsoAid Advantage IAI-125A) from scenario #1 to scenario #6 in order G) Heterogeneity correction factors (HCFs) for the lens for a 16-mm 125I COMS plaque (model: IsoAid Advantage IAI-125A) for scenario #7
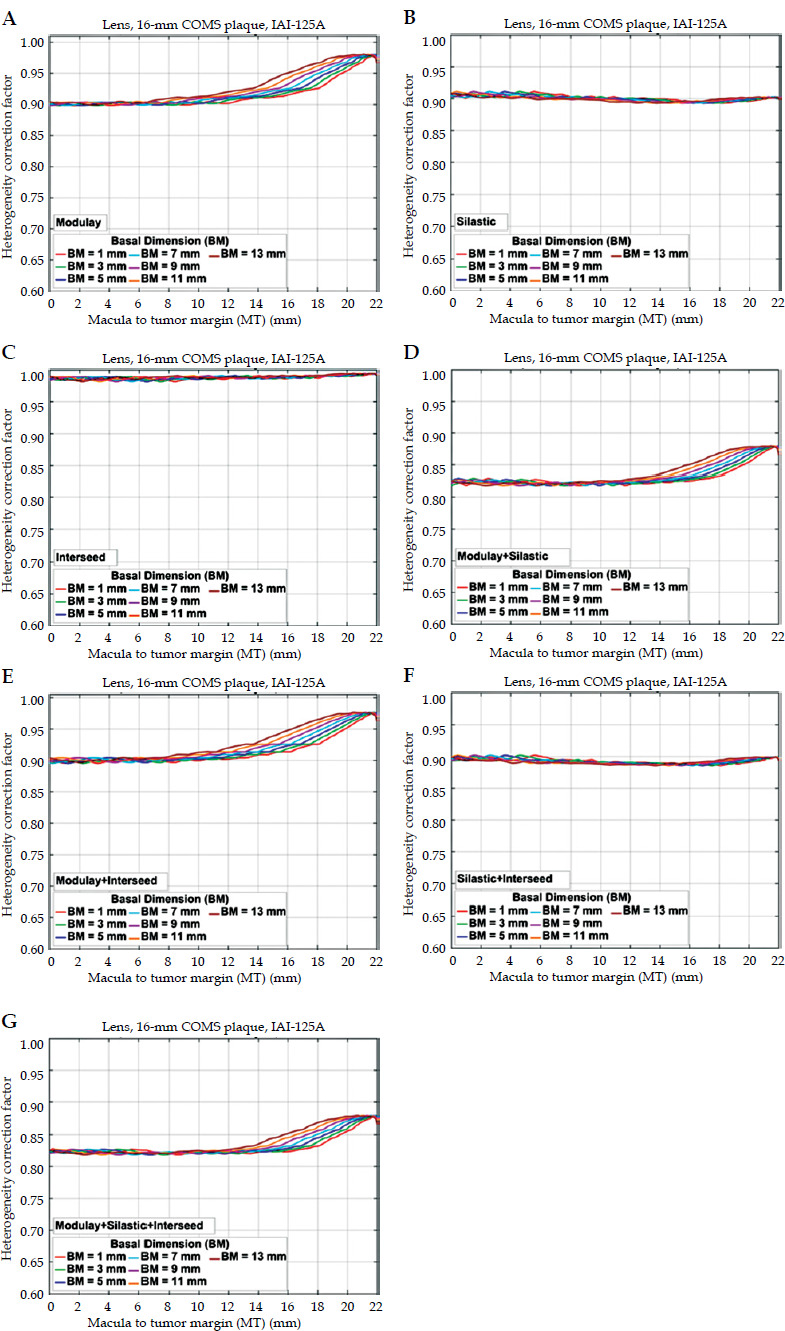
Like those for the macula, dominant contributing factors for the lens were the Modulay backing and Silastic insert, and their dominancy was MT- and BM-dependent (Figure 4). At MT ≤ 21.1 mm for BM of 1 mm, at MT ≤ 20.8 mm for BM of 3 mm, at MT ≤ 20.5 mm for BM of 5 mm, at MT ≤ 20.1 mm for BM of 7 mm, at MT ≤ 19.6 mm for BM of 9 mm, at MT ≤ 19.1 mm for BM of 11 mm, and at MT ≤ 18.5 mm for BM of 13 mm, the contributing factors were both the Modulay backing and Silastic insert (range, 12.8-18.2%). At farther MT, the effect of Modulay backing was small (≤ 3%) and hence, the Silastic insert was the key factor (range, 8.9-10.0%).
HCFs for central axis and off-axis points for seven scenarios: The other six COMS plaques
The ranges of central axis HCFs for the other six 125I COMS plaques (10-14 mm and 18-22 mm) are presented in Table 3 from scenario #1 to scenario #7 in order. Central axis HCFs for the other six plaques showed similar trends to those for the 16-mm plaque, but their magnitudes were slightly different (data not shown here). Maximum absolute HCF differences from the 16-mm plaque were 0.037 (10-mm plaque, occurred in scenario #7 at a depth of 0 mm), 0.024 (12-mm plaque, scenario #7 at 0 mm), 0.017 (14-mm plaque, scenario #7 at 0 mm), 0.009 (18-mm plaque, scenario #3 at 15 mm), 0.009 (20-mm plaque, scenario #6 at 11 mm), and 0.013 (22-mm plaque, scenario #2 at 20 mm). It was observed that dose enhancement by Modulay backing alone (#1) at a depth ≤ 1 mm increased as decreasing plaque size: 1.8% (10-mm plaque), 1.5% (12-mm plaque), 1.2% (14-mm plaque), 0.8% (16-mm plaque), 0.5% (18-mm plaque), 0.4% (20-mm plaque), and 0.2% (22-mm plaque).
Table 3
Ranges of central axis and off-axis heterogeneity correction factors (HCFs) for the other six COMS plaques (10-14 mm and 18-22 mm) loaded with 125I seeds (model: IsoAid Advantage IAI-125A) for seven scenarios (#1-#7)
The ranges of off-axis HCFs for the other six 125I COMS plaques (10-14 mm and 18-22 mm) are presented in Table 3 from scenario #1 to scenario #7 in order. For the optic disc (or macula), the ranges of HCFs for Modulay backing alone (#1) for 10-, 12-, and 14-mm plaques were much greater (by 0.113, 0.166, and 0.129, respectively) than those for the 16-mm plaque, but those for 18-, 20-, and 22-mm plaques were slightly smaller (by 0.005, 0.014, and 0.016, respectively). On the other hand, HCFs for the other six plaques (10-14 mm and 18-22 mm) had relatively comparable ranges with those for the 16-mm plaque within 0.008 for Silastic insert alone (#2), and within 0.004 for interseed effects alone (#3). For the lens, the ranges of HCFs for Modulay backing alone (#1) for 10-, 12-, and 14-mm plaques were slightly greater (by 0.016, 0.012, and 0.008, respectively) than those for the 16-mm plaque, and those for 18-, 20-, and 22-mm plaques were slightly smaller (by 0.001, 0.006, and 0.011, respectively). HCFs for the other six plaques had similar ranges to those for the 16-mm plaque within 0.006 for Silastic insert alone (#2) and within 0.004 for interseed effects alone (#3). Since maximum and minimum HCFs occurred at different DT (or MT) for each plaque, the maximum absolute HCF differences between the other plaque(s) and the 16-mm plaque calculated at the same DT (MT) for each BD (BM) were greater than the absolute differences in ranges between the other plaque(s) and the 16-mm plaque. The maximum absolute HCF differences between 10-mm and 16-mm plaques for the optic disc (or macula) and lens were 0.188 and 0.024. Corresponding values were 0.211 and 0.020 (between 12-mm and 16-mm), 0.152 and 0.012 (between 14-mm and 16-mm), 0.051 and 0.013 (between 18-mm and 16-mm), 0.083 and 0.016 (between 20-mm and 16-mm), 0.099 and 0.021 (between 22-mm and 16-mm). The maximum differences occurred in scenario #1.
Discussion
The unique trends of central axis HCFs for the seven scenarios presented in Table 2 are attributed to the effective atomic numbers and physical densities of the Modulay backing and Silastic insert as well as the low average photon energy (~28 keV) from 125I seeds used in this study (dominant photo-electric effect). The slight dose enhancement (up to 0.8%) by the Modulay backing near the seeds and plaque is consistent with the result reported by Thomson et al. [17]. The phenomenon is due to fluorescence photons emitted from atoms in the Modulay backing when the atoms are excited by photons from the 125I seeds and subsequently, relax to a ground state [17]. The continuous dose reduction with depth by the Modulay backing is due to enhanced photo-electric absorption and decreased Compton scatter by high-Z material of the Modulay backing relative to water in the low energy photon [17]. The large dose reduction (range, 9.0-13.8%) by the Silastic insert relative to water is attributable to photon attenuation by the Silastic insert, which has a higher effective atomic number (Zeff ~10.7) than water (Zeff ~7.4). At a shallow depth, photons from seeds in off-axis locations travel through thicker Silastic insert than those from the central axis seed, resulting in substantial attenuation (13.8% or less) [17]. At a deeper depth, the difference in Silastic insert thickness to travel between central axis and off-axis seeds decreases and hence, attenuation decreases and eventually becomes constant (~9.0%). Our result (i.e., constant HCF at a deeper depth) is consistent with the result for a single 125I seed by Thomson et al. [17]. Interseed attenuation is small because the seeds in COMS plaques are not in positions in line with multiple seeds like those in prostate brachytherapy [17]. While Thomson et al. reported ~1% of the interseed effect for fully loaded 12-, 16-, and 20-mm 125I COMS plaques, Zhang et al. stated up to 4% for a fully loaded 16-mm 125I COMS plaque [17, 18]. Because of the small interseed effect (≤ 1.7%) investigated in this study, HCFs for Modulay backing + Silastic insert (scenario #4) are comparable to HCFs for Modulay backing + Silastic insert + interseed effects (scenario #7) (Table 2).
For central axis HCFs, any combined effect of contributing factors (scenarios, #4-#7) can be computed from the superposition of individual contributing factors (within 3.3%). For example, HCFs for scenarios #1, #2, and #4 at a depth of 5 mm are 0.970, 0.905, and 0.878, respectively (Table 2). The absolute difference between multiplication (= 0.8779) of HCF for scenario #1 and HCF for scenario #2 and HCF (= 0.878) for scenario #4 is 0.0001. For most cases, the difference is < 3%. Maximum absolute differences are usually observed in the combined effect of all three factors at a deep depth ≥ 15 mm, and they are 0.021 (10-mm plaque), 0.023 (12-mm plaque), 0.017 (14-mm plaque), 0.025 (16-mm plaque), 0.029 (18-mm plaque), 0.033 (20-mm plaque), and 0.022 (22-mm plaque).
This study identified dominant factor(s) to central axis heterogeneity corrections at a particular depth for the 16-mm 125I COMS plaque (Table 2). At a depth ≤ 5 mm, the Silastic insert is the most dominant contributing factor (range, 9.5-13.8%) because the effects of Modulay backing and interseed effects are relatively small (≤ 3.0% and ≤ 0.7%, respectively). Zhang et al. also supported the great impact of Silastic insert at a shallow depth [18]. At a depth > 5 mm, the effects of Modulay backing and Silastic insert are greater than 3.0% and hence, both are contributing factors (range, 12.2-19.0%). These depth-dependent dominant factors ultimately determine the unique trend of HCF for the combined effect of all three factors (i.e., HCF increases, reaches the maximum, then decreases with depth) (Figure 1).
The trends of HCFs for the optic disc (macula) for the seven scenarios have a dependence on DT (MT) and BD (BM) (Figures 2 and 3). The dose enhancement (up to 0.9%) at DT (MT) ≤ 6.2 (6.9) mm and the further dose reduction at DT (MT) ≤ 10 (11) mm by Modulay backing alone (#1) (Figures 2A and 3A) are attributed to the same reasons (i.e., fluorescence photons, enhanced photo-electric absorption, and decreased Compton scatter) as explained above for the central axis HCFs. At DT (MT) ≤ 6.2 (6.9) mm, the farthest DT (MT), where constant dose enhancement ends, decreases as increasing BD (BM) because the optic disc (macula) becomes farther from the plaque center as increasing BD (BM) (Figures 2A and 3A). At DT (MT) > 10 (11) mm, the dose reduction reaches the maximum and becomes constant because the optic disc (macula) becomes farther from the plaque edge, and photo-electric absorption and Compton scatter decrease and reach the minimum (Figures 2A and 3A). The high attenuation by Silastic insert alone (#2) results in a dose reduction of 9.1-15.3% (Figures 2B and 3B). The unique trend of HCFs for Silastic insert alone (#2) would be related to Silastic insert thickness that photons from each seed travel through, and eye curvature. As an example, for BD (BM) of 13 mm, when the optic disc (macula) is near the plaque edge (DT (MT) ≤ 2 mm), photons from far seeds travel through thicker Silastic insert, and the overall attenuation/dose reduction becomes greater. As the optic disc (macula) becomes farther from the plaque edge (i.e., as DT (MT) increases along the eye) and Silastic insert thickness to travel through decreases, the attenuation/dose reduction decreases and reaches the minimum (i.e., HCF increases and becomes constant). Interseed attenuation is small for the same reason as delineated above for the central axis HCFs (Figures 2C and 3C). For the same reason (i.e., small interseed effect (≤ 2.3%)) as for central axis HCFs, scenario #4 is comparable to scenario #7 for the optic disc (macula) (Figures 2D, G, and 3D, G). The same trends and ranges for the macula as those for the optic disc are due to the spherical shape of the eye, but the same trends occurring at slightly different MT are due to different coordinates between the optic disc and the macula.
The trends of HCFs for the lens for the seven scenarios are different from those for the macula (Figures 3 and 4). The different trends are attributed to the location of the lens with respect to the macula. Since the lens is in the opposite to the macula, the trend of dose reduction with MT by Modulay backing alone (#1) is opposite to that for the macula (Figures 3A and 4A). The attenuation/dose reduction by Silastic insert alone (#2), however, is almost constant (range, 8.9-10.7%) for all BMs at MT ≤ 22 mm (Figure 4B) because the lens is far enough from the plaque. The trend of HCFs for interseed effects alone (#3) for the lens is also opposite to that for the macula for a similar reason (i.e., location of the lens) (Figure 3C and 4C). Similarly, scenario #4 is comparable with scenario #7 for the lens (Figure 4D, G).
Additionally, for off-axis HCFs, the combined effects of contributing factors (scenarios, #4-#7) are relatively comparable with the superposition of individual contributing factors. For the optic disc, macula, and lens, the maximum absolute differences between any combined effect and superposition for all BDs or BMs at DT or MT ≤ 22 mm for all seven plaques are the greatest (3.5% for the optic disc, 3.9% for the macula, and 2.7% for the lens) in the combined effect of all three factors (#1 × #2 × #3 vs. #7), followed by the effects of Modulay backing + Silastic insert (#1 × #2 vs. #4)/Modulay backing + interseed effects (#1 × #3 vs. #5) (2.4% for the optic disc, 2.4% for the macula, and 1.7% for the lens), and Silastic insert + interseed effects (#2 × #3 vs. #6) (1.8% for the optic disc, 1.8% for the macula, and 1.0% for the lens).
The current study also identified dominant factor(s) to off-axis heterogeneity corrections at particular DT (MT) for each BD (BM) (Figures 2-4). For a similar reason (i.e., small contributions from the Modulay backing and interseed effects) to that for central axis heterogeneity corrections described above, for the optic disc (macula), the Silastic insert is the most dominant factor (≥ 11.8%) at close DT (MT) ≤ 6.9 (7.6) mm, and both the Modulay backing and Silastic insert are contributing factors (range, 18.3-24.4%) at farther DT (MT). For the lens, due to its location relative to the macula, the Silastic insert is the primary factor (range, 8.9-10.0%) at far MT > 18.5 mm, and both the Modulay backing and Silastic insert are the contributing factors (range, 12.8-18.2%) at MT ≤ 18.5 mm.
The same trends but different magnitudes of central axis HCFs for the seven scenarios are observed for the other six 125I COMS plaques (10-14 mm and 18-22 mm). The same trends of central axis HCFs for the other six plaques as for the 16-mm plaque are due to the same reason (i.e., effects of Modulay backing, Silastic insert, and interseed effects) described above for the 16-mm plaque. The different magnitudes are attributed to different plaque sizes (different number and configuration of seeds) affecting fluorescence photons, photo-electric absorption, and Compton scatter by the Modulay backing, and photon attenuation by the Silastic insert. For example, dose enhancement by the Modulay backing alone (#1) near the seeds and plaque increases as decreasing plaque size, because seeds in smaller plaques are closer to the central axis and more fluorescence photons reach to the central axis.
The much greater ranges of the optic disc (or macula) HCFs for Modulay backing alone (#1) for 10-, 12-, and 14-mm plaques are due to smaller plaque sizes (Table 3). The minimum and maximum values of HCFs are smaller and greater, respectively, for the three plaques than those for the 16-mm plaque, resulting in greater ranges of HCFs. The greater maximum values of HCFs near the seeds and plaque for those three plaques are due to more fluorescence photons reaching to the optic disc (or macula) (shorter distance from seeds to the optic disc (or macula)). The smaller minimum values of HCFs at short DT (MT) for the three plaques are due to more photo-electric absorption (shorter distance from seeds) and less Compton scatter (smaller sizes of plaques).
The findings of this study will help improve the current clinical practice and design new eye plaques. The current clinical practice for dosimetry of COMS plaques is a dose calculation based on TG-43 assumptions, which greatly overestimates central axis and off-axis point doses [16]. However, currently, there is no Food and Drug Administration-approved MC-based treatment planning system available [16]. In addition, implementing an MC-based open-source tool is a tedious process, and accurate calculations require high-performing computers and a long computational time [16]. Therefore, an alternative method of estimating heterogeneous dose is to use HCFs, which can be multiplied by homogenous dose (TG-43 formalism-based calculations) as recommended by the AAPM TG 221 [11]. The current study demonstrated that dominant contributing factors to heterogeneity corrections are the Modulay backing and Silastic insert, and their contributions are not negligible. From these findings, one can identify a single dominant contributing factor for his/her own clinical case and estimate heterogeneous dose efficiently. For example, one universal HCF value for the dominant Modulay backing effect is 0.9 for the optic disc (Figure 2A), macula (Figure 3A), and lens (Figure 4A) at DT > 10 mm, MT > 10 mm, and MT < 10 mm, respectively. Furthermore, this study provides guidance on designing new eye plaques. As an example, plaques can be devised without the Silastic insert to reduce dose perturbation within 10 mm from the plaque (Figures 1, 2B, 3B, and 4B), like Eye Physics plaques [23]. Knowing the large HCFs for the Modulay backing, a different material with a lower density (e.g., titanium) than gold can be utilized to reduce heterogeneity effect. Using titanium will permit patient-specific CT imaging without a severe metal artifact and ultimately, CT-based planning.
Conclusions
This study determined the magnitudes of individual contributing factors to central axis and off-axis heterogeneity corrections for 125I COMS plaques, and identified the dominant contributing factor(s) at a particular depth (central axis) and at specific DT or MT for each BD or BM (off-axis). For the 16-mm COMS plaque, at a depth ≤ 5 mm, the major contributing factor to central axis heterogeneity corrections is the Silastic insert (dose reduction by 9.5-13.8% with heterogeneity), whereas at a depth > 5 mm, both the Modulay backing and Silastic insert are contributing factors (range, 12.2-19.0%). For the optic disc (macula), at short DT (MT) for each BD (BM) (e.g., at DT (MT) ≤ 0.6 (1.4) mm for BD (BM) of 13 mm)), the Silastic insert is the most predominant factor (≥ 11.8%) to off-axis heterogeneity corrections but at farther DT (MT), both the Modulay backing and Silastic insert are contributing (range, 18.3-24.4%). For the lens, due to its location with respective to the macula, at far MT > 18.5 mm, the Silastic insert is the most contributing factor (range, 8.9-10.0%) but at MT ≤ 18.5 mm, both the Modulay backing and Silastic insert are primarily contributing (range, 12.8-18.2%). In both central axis and off-axis heterogeneity corrections, the interseed effect is small (≤ 1.7% and ≤ 2.3%, respectively). Data for the other six plaques (10-14 mm and 18-22 mm) are relatively similar to those for the 16-mm plaque, except that for the optic disc (or macula), the Modulay backing effects for 10-, 12-, and 14-mm plaques are much greater than that for the 16-mm plaque by 0.188 (18.8%), 0.211 (21.1%), and 0.152 (15.2%), respectively. The use of universal HCF(s) for the two dominant factors (Modulay backing and Silastic insert) determined in this study will facilitate heterogeneous dose estimates for each clinical scenario without an MC tool.