

Purpose
Brachytherapy is a versatile treatment that delivers highly concentrated doses of radiation to tumor targets while limiting dose to surrounding organs at risk. It can conveniently be given in a single-session using low-dose-rate brachytherapy (LDR-BT), whereas high-dose-rate brachytherapy (HDR-BT) is more traditionally applied over multiple treatment fractions. HDR-BT does have planning advantages over LDR-BT in that the dose that will be delivered can be determined prior to its’ delivery, and the patient does not need to go home with any radioactive seeds. Whether HDR-BT can be delivered as a single-fraction treatment with similar oncologic outcomes and acute/late toxicities as multi-fractionated regimens, is not well-known.
The purpose of this study was to review the literature on single-fraction HDR brachytherapy for the treatment of all disease sites, to evaluate the extent of published literature on this topic.
Material and methods
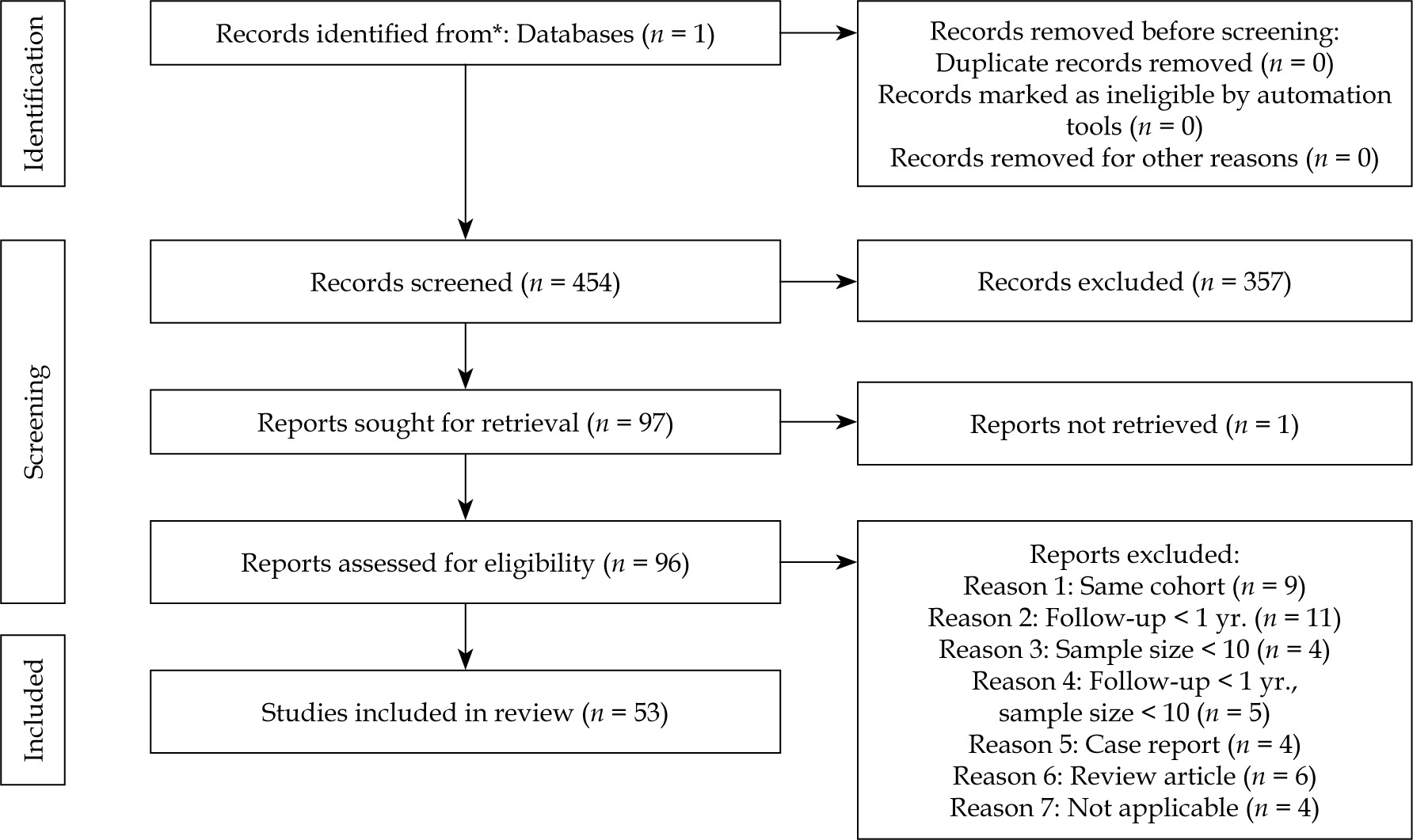
A scoping review was performed using the PubMed database, and according to the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines. The PubMed database was queried with the following search terms from 1994-2021: ‘brachytherapy’, which generated 26,899 results, ‘high-dose-rate’, which generated 5,356 results, and ‘single-fraction’, which generated 56,908 results. A combined search of ‘brachytherapy AND high-dose-rate AND single-fraction’, yielded 454 results.
The results were reviewed by three authors for inclusion/exclusion (MK, SN, and MK). From the initial 454 records for review, 357 were excluded as they were irrelevant, they were dosimetry studies, or multi-fraction treatments. As a result, 97 reports were sought for retrieval, of which one was not retrieved as the full article was not available on PubMed. From the 96 reports that were assessed for eligibility, 43 papers were excluded for the following reasons: 9 had the same cohort, 11 with follow-up less than 1 year, 4 with sample size less than 10 patients, 5 reports with combination of both follow-up less than 1 year and sample size less than 10 patients, 4 case reports, 6 review articles, and 4 studies that were not applicable. Therefore, 53 studies were included in the final scoping review (Figure 1).
Prostate
Clinical outcomes
Seventeen studies (14 definitive, 1 focal definitive, and 2 focal salvage) with 1,474 patients reported on single-fraction treatment between 2016-2021 (Table 1). Six studies were from the UK, 3 from the USA, 3 from Spain, 3 from Canada, 1 from the Netherlands, and 1 from Italy. Single-fraction dose delivered ranged from 19 to 21 Gy. Eight studies treated patients with androgen deprivation therapy treatment over a range between 3 and 36 months. In the definitive therapy series, median follow-up ranged from 20 to 72 months, while in the salvage series it ranged from 25 to 26 months [1-17].
Table 1
Single-fraction prostate high-dose-rate brachytherapy (HDR-BT) studies
Of the 14 studies that treated patients with definitive intent, prostate specific antigen (PSA) control rates ranged from 65 to 94% (Figure 2). Seven studies stratified PSA control based on risk groups. PSA control rates for low-risk patients ranged from 79% to 100%, for intermediate-risk patients ranged from 75% to 86%, and for high-risk patients ranged from 75% to 76% (Figure 3).

Fig. 3
Risk stratified biochemical control rates in singlefraction prostate cancer definitive treatment studies

The most significant study reported was a randomized controlled trial of single-fraction 19 Gy vs. two fractions of 13.5 Gy [18]. This study included 170 patients with either low- or intermediate-risk, with no prior androgen deprivation therapy. Median follow-up was 60 months. The study resulted in a significantly higher rate of PSA biochemical failure in the single-fraction arm. G3 genitourinary (GU) toxicity was only seen in 3% in the single-fraction arm and no reported cases in the two-fraction arm; however, this was statistically insignificant between both groups.
When reviewing patterns of failures after single-fraction treatment, high rates of local failures were reported in a dominant intra-prostatic lesion. Studies that reported on local failure rates reported that this occurred in 4-78% of cases. Attempts to reduce failures in the dominant intra-prostatic lesion by increasing the single-fraction dose have not been successful to date. Prada et al. increased the whole gland single-fraction dose to 20.5 Gy [9], and Armstrong et al. performed a focal boost of 21 Gy to the dominant intra-prostatic lesion [2], but there were still higher than expected failures compared with a multi-fraction regimen. For patients treated with salvage treatment, two studies reported on outcomes with 2-year PSA control rates ranging from 42% to 59%. These results, similar to the definitive setting, demonstrated less than ideal outcomes with single-fraction treatment [12, 16].
Toxicities
Acute G1-G2 GU toxicities were reported in 0-12%, while acute G1-G2 gastrointestinal (GI) toxicities were reported in 0-3% of patients. Acute G3 or higher GU or GI toxicities were reported in 0%. Late G1-G2 GU toxicities were reported in 0-60%, while late G1-G2 GI toxicities were reported in 0-6%. Late G3 or higher GU or GI toxicities were reported in 0-6%. Types of late G3 toxicities reported were urethral strictures [2], rectal fistulae [14], chronic diarrhea [11] that was medically managed, and obstruction of the urinary tract that necessitated TURP [1].
Breast
Seven studies (all definitive after lumpectomy) with 268 patients were reporting on receiving single-fraction treatment between 2008-2021 (Table 2). Five studies were from France, 1 from Spain, and 1 from the USA. Single-fraction high-dose brachytherapy dose delivered ranged between 16 and 21 Gy. Median ages of patients treated ranged from 64 to 77 years, and included patients with early-stage breast cancer [18-24].
Table 2
Single-fraction breast high-dose-rate brachytherapy (HDR-BT) studies
[i] LR – local recurrence; DFS – disease-free survival; OS – overall survival; 1the first 18 patients were treated with a single-fraction dose of 20 Gy; 2given high rates of acute toxicities with 20 Gy, the remaining 34 were treated with a single-fraction dose of 18 Gy; 3the paper did not distinguish between the G3 events in the hyper-fractionated and single-fraction group
Median reported follow-up ranged from 24 to 72 months. At 6 years, freedom from local recurrence (LR) was 100%, disease-free survival (DFS) ranged from 82% to 100%, and median overall survival (OS) ranged from 82% to 100%.
Toxicities
Single-fraction treatment appeared to be well-tolerated in acute and late term settings. Amongst the doses used, Sacchini’s paper initially assessed a single-fraction dose of 20 Gy. However, due to increased acute toxicity rates, the dose was lowered to 18 Gy [24]. This is also a unique series that used an HDR applicator intra-operatively, and the dose distribution with this approach was very different from that of the other papers, which used an interstitial technique. For papers that used doses in the 16-18 Gy range, serious acute toxicities were seen in < 5% of patients. No grade 3 or higher late toxicities have been reported to date. Excellent to good cosmesis outcomes were reported in 76-98% of patients. These early to mid-term results of single-fraction brachytherapy appear promising for this highly selected group of favorable patients. Longer term data is needed to confirm the favorable oncologic and cosmetic results.
Liver
Eighteen studies (7 primary, 11 metastasis) with 618 patients have been reported on receiving single-fraction treatment between 2004-2021 (Table 3). Seventeen studies were from Germany, and one was from Poland [25-42]. Single-fraction high-dose brachytherapy dose delivered ranged from 8 to 25 Gy. Median follow-up range for series that treated a primary liver cancer was 12-23 months, and median follow-up range for series that treated liver metastasis ranged from 11 to 28 months. Local control range for primary disease ranged from 37% to 93%, and local control range for metastasis ranged from 40% to 94% (Figure 4). Furthermore, Denecke et al. focused on comparing single-fraction brachytherapy as a bridge to liver transplant compared with the standard modality of transarterial chemoembolization (TACE). This study showed that for patients who are not candidates for TACE, single-fraction treatment may be an acceptable alternative modality [28]. There are large variations in the local control rates reported. Much of this seems to be related to the dose given as well as the size of the tumor treated. Ricke et al. showed in a dose escalation trial, for example, improved local control rates when increasing the dosage from 15 Gy to 25 Gy in a single-fraction [33].
Table 3
Single-fraction liver high-dose-rate (HDR) studies
[i] LTC – local tumor control; PFS – progression-free survival; OS – overall survival; 1mean age; 2mean or minimum; 3median volume (cm3); 4local recurrence rates were better with brachytherapy compared with trans-arterial chemo-embolization, 5unspecified if PFS rates applied to one or all three groups were evaluated, 6unspecified if OS rates were from high-dose-rate (HDR) brachytherapy alone or HDR + laser-induced thermal treatment, 78 of 10 patients with local tumor progression died from poor liver function, 8unspecified if complications occurred in single-fraction or fractionated groups (2 cases of intra-abdominal hemorrhage, and 1 case of Gram-negative septicemia); 9abscesses secondary to ascending biliary infection in patients who underwent Whipple’s or pylorus-preserving resection of pancreatic head in patients with biliodigestive anastomosis; 101 of 3 patients with biliodigestive anastomosis developed hepatic abscess 4.9 months post-ablation

Toxicities
G3 toxicity was reported in 3 patients with liver abscesses post-interstitial brachytherapy in a study done by Drewes et al. [29]. Other serious complications were noted, including post-interventional abdominal hemorrhage, pneumothorax, biliary abscess [41], and Gram-negative septicemia [38]; however, only a few cases were reported with such complications (Table 3). Overall single-fraction HDR-BT appeared to be a safe modality given a low number of serious toxicities reported to date.
Other cancers
Eleven published studies met the inclusion criteria in assessing the efficacy of single-fraction high-dose brachytherapy for cancers other than prostate, breast, and liver. The studies were published by groups in the following locations: 4 from the USA, 3 from Germany, 1 from Italy, 1 from the United Kingdom, 1 from China, and 1 from Spain [43-53]. Table 4 summarizes the oncological outcomes and toxicities for these eleven publications. There were 3 studies for gastrointestinal, 2 studies for head and neck, 3 studies for lung, 1 study for gastrointestinal stroma tumor, 1 study for glioma, and 1 study for endometrial carcinoma. Amongst these studies, lung appears to have promising data. Yoon et al. reported on 23 patients treated with 21.5 Gy single-fraction HDR brachytherapy, with local control of 96% at 2 years for centrally located primary and metastatic lung cancer, and no G3 or higher toxicities were reported [52]. Xiang et al. also reported on single-fraction HDR lung brachytherapy in a phase I clinical trial. A single-fraction of 30 Gy brachytherapy to the primary in combination with intensity-modulated radiation therapy (IMRT) to nodal regions while receiving concurrent chemotherapy resulted in 82% local tumor control at 2 years [51]. It is difficult to make any definite conclusions regarding the efficacy of single-fraction brachytherapy for lung or these other less common sites, given the limited data for each type of cancer.
Table 4
Single-fraction other sites high-dose-rate brachytherapy (HDR-BT) studies
[i] LTC – local tumor control; PFS – progression-free survival; OS – overall survival; 1mean age; 2mean size; 3mean dose; 4mean follow-up; 5one year PFS was 91% for patients treated with dose > 15 Gy, and 61% for patients treated with a dose < 15 Gy; 6patient was previously treated with a Hartmann procedure and developed a fistula; 7patient previously had ulceration in the perineal region secondary to the tumor and developed an abscess; 8patient was successfully treated with transcutaneous drainage and antibiotics; 9patient required embolization with digital subtraction angiography; 10patient required treatment with a pleural drain; 11gross tumor volume with single-fraction HDR-BT; 12PTV using IMRT
Discussion
There is interest in single-fraction treatment both from a patient and hospital system perspectives. Increasing studies are being conducted using single-fraction external beam treatments [54], including randomized clinical trials. Brachytherapy is uniquely positioned to deliver very high doses of radiation in single treatments with rapid fall-off, and may provide various advantages over external beam approaches. Delivering a single-fraction HDR brachytherapy is technically feasible, but there are unanswered questions regarding the safety and efficacy of delivering very high doses of radiation in a single treatment. Determining whether pursuit of such an effort is worthwhile requires an understanding of the current published literature on this topic.
Our literature search identified 53 papers, which were included in this review. A large number of prostate cancer patients have been treated with single-fraction treatment and mostly in the definitive setting. There has even been a randomized controlled trial on two versus single-fraction HDR-BT demonstrating inferior biochemical control in the single-fraction arm [55]. Multiple studies also demonstrate high rates of locally persistent disease predominantly in the dominant intra-prostatic lesion [56]. Further attempts at single-fraction dose escalation has also not significantly improved outcomes [1]. In addition, in reviewing the biochemical control outcomes by risk group, it does not appear that there is a risk group that has acceptable control with single-fraction treatment. Based on the current literature, it does not appear that single-fraction HDR-BT for definitive prostate cancer treatment is an acceptable standard of care. Any future work in this area should be conducted as part of a clinical trial.
The published work on single-fraction treatment in the salvage setting is limited to just two studies, but the overall trends are similar as that seen in the definitive setting, with worse than expected biochemical control compared with multi-fractionated regimens. It seems likely that single-fraction treatment in the salvage setting will also not be ideal regarding long-term oncologic control. The reasons for these less than promising results is not entirely clear. It likely includes an incomplete understanding of radiation biology and accurate conversions of dose using α/β ratio and linear quadratic modelling as well has cell re-assortment and hypoxia. These limitations should be balanced with the possible lower toxicities seen in the short-term with a single-fraction treatment, which is a more pertinent consideration in the re-irradiation setting. However, longer follow-up is needed with single-fraction regimens in this setting. As in the definitive setting, worse GU toxicities have been reported with single- vs. multi-fraction regimens [4].
Single-fraction breast literature appears promising both in terms of early oncologic control and limited toxicities. It is difficult to know whether the high local control rates confirm that single-fraction treatments are truly effective, or whether the relatively low-risk population would not have recurred even without adjuvant radiation. The experience with single-fraction treatment is also mostly limited to one group in France that has used an interstitial technique. There is an ongoing clinical trial with a balloon-based single-fraction technique, which has not reported oncologic outcomes yet [57], but has reported limited severe toxicities to date. Single-fraction external beam treatments are also being developed both in the pre-operative and post-operative spaces [58]. Continued work in this space is needed to determine the ideal single-fraction dose, and long-term oncologic and toxicity outcomes. It is important for future studies to include prospective collection of quality-of-life data, as these would be necessary to understand the place of brachytherapy compared with alternative external beam methods for delivering single-fraction doses.
Single-fraction liver treatments have been published in retrospective, single-arm prospective, and even in randomized controlled trials [59]. Liver single-fraction literature is unique in that dose escalation trials have been performed to find the ideal dose, as previously mentioned in a study by Ricke et al. [33]. Significant work has also been done to determine organ at risk dose constraints, and understanding of the limitations of treating perihilar disease. Local control rates for appropriately sized lesions treated with appropriate single-fraction doses demonstrate local control ranges comparable to stereotactic body radiation therapy or other ablative techniques. Toxicities also seem limited. According to the 2018 ESMO guidelines for hepatocellular cancer, single-fraction liver brachytherapy is now included as a treatment option. These encouraging results in the liver are despite the fact that many patients were heavily pre-treated, and had failed other prior local therapy regimens.
Additional single-fraction studies have been done outside of the prostate, breast, and liver, but are very limited. There is some promising data in the lung, but overall conclusions are limited given the small numbers of patients who have been treated to date.
Our study has some limitations. PubMed was the only queried database, and if we had conducted a systematic review and included additional databases, we may have found more studies. Also, not all studies provided the same categories of data, such as prostate risk groups, which made it more challenging to evaluate certain patients’ sub-groups.
Conclusions
The medium-sized body of literature published on single-fraction HDR brachytherapy shows this modality as safe, but its’ efficacy varies amongst different disease sites. Breast and liver have the most promising data, while prostate has the least encouraging, and conclusions are limited with respect to other cancers. Additional prospective evaluation of single-fraction HDR-BT studies is warranted.