Introduction
During the last years many modifications of standard dialysis access steal-correcting techniques have been reported. Additionally, new endovascular options have joined the armamentarium.
Aim
We reviewed the English literature, and we report the most popular techniques included in a step-by-step approach to deal with dialysis access steal syndrome (DASS).
Material and methods
We searched for all studies including case reports, observational studies and interventional trials that reported intra-operative techniques to treat DASS. We considered studies published from January 1990 until April 2022. We included studies published only in English language. A systematic search for related studies was done on PubMed and Cochrane Database and the last search date was April 30, 2022. Search terms were “Arterio-venous fistula” OR “AVF” OR “Hemodialysis Access” OR “AVBG” OR “Brachiocephalic fistula” OR “Basilic vein transposition” OR “Brachio-basilic fistula” AND “Dialysis access steal syndrome” OR “Steal syndrome” OR “Ischemia”. Information such as first author’s name, journal, year of publication, country of origin, intra-operative technique used, and site of arteriovenous fistula was extracted from studies.
Results
A total of 396 studies were retrieved after applying this search strategy. Two-hundred and twenty two were excluded because they were not relevant to the scope of this review. From the remaining 174 studies, 20 were chosen as more representative of the full spectrum of the currently used techniques. The majority of studies were retrospective case series or case reports. Briefly, intraoperative techniques described were variable: a) banding or plication, b) short graft interposition, c) revision using distal inflow (RUDI), d) distal revascularization with interval ligation (DRIL), e) proximalization of arterial inflow (PAI), f) prolongation of existing grafts, g) distal radial artery ligation (DRAL), h) anastomosis reduction, and i) ligation. These results can help vascular surgeons in decision making regarding the most applicable technique in every DASS patient.
Discussion
For every patient who is a candidate for arteriovenous access formation, we proceed with a stepwise approach to minimize the risk of DASS. The first step is to take a history for the presence of diabetes, atherosclerosis, current or past use of central catheters, defibrillators or pacemakers. The second step is to perform a detailed physical examination, including palpation of radial pulses and blood pressure measurement in both upper extremities. A difference > 20 mm Hg is indicative of inflow stenosis, which must be corrected. An absent radial pulse does not preclude access formation. Consequently, we perform an Allen test, which may be aided with a hand-held Doppler and/or a pulse oximetry [1]. An abnormal test puts the patient in the high-risk group for DASS. Color Duplex ultrasound (CDU) is performed to gain anatomical information about upper arm venous size, patency and distensibility as well as arterial wall calcification and lumen patency. Based on the physical examination we perform selectively a preoperative angiogram with simultaneous angioplasty of any proximal subclavian or distal arm stenoses [2]. In the case of arm edema, prominent arm and/or chest veins or history of central venous catheter, venography is performed.
After AVA creation, if symptoms suspicious for DASS emerge acutely or in the long term, we proceed with physical examination. Compression of the AVA beyond the anastomosis restores radial pulses in case of absence. If not, severe forearm (or juxta-anastomotic) stenotic lesions must be suspected. Therefore, compression of the arterio-venous fistula (AVF) relieves the symptoms and restores the pulses if high flow is the only cause of DASS. Some consider that doubling of the digital waveform amplitude is considered diagnostic for DASS. Digital blood pressure (DBP) < 60 mm Hg and a digital brachial index (DBI) < 0.45 may detect DASS [1]. Oxygen saturation < 94% is associated with DASS and intraoperative normalization indicates correction of steal [3]. CDU determines if the access is normal or over-functioning. Access flow is closely represented from the brachial flow, which is measured 5 cm proximal to the anastomosis. Thus, the probe is placed away from the turbulent anastomotic flow. Afterwards, digital subtraction angiography (DSA) is performed to examine the presence of atheromatic stenoses or distal microangiopathy [2]. Percutaneous transluminal angioplasty (PTA) is indicated to correct any proximal stenotic lesions or lesions distal to the anastomosis. This maneuver may treat steal in nearly all patients with disease above the elbow but for below the elbow nearly half of the patients need secondary surgical intervention [2]. After manual closure of the AVF, an angiographic blush sign is considered essential to predict ulcer healing in the distal arm [4]. If symptoms persist, we proceed with ligation of any significant venous side-branches, if they are apparent in an AVF, to increase venous outflow resistance. Alternatively, transcatheter coil embolization may be performed.
If needed, we may proceed with more specialized procedures such as: a) banding or plication, b) short graft interposition, c) revision using distal inflow (RUDI), d) distal revascularization with interval ligation (DRIL), e) proximalization of arterial inflow (PAI), f) prolongation of existing grafts, g) distal radial artery ligation (DRAL), h) anastomosis reduction, and i) ligation. Banding, short graft interposition and RUDI are suggested for high-flow while DRIL, modified DRIL and PAI are suggested for normal-flow AVAs [3]. In some cases without arm ischemia, high-flow (> 2000 ml/min) has to be reduced to prevent or restore adverse AVF-induced cardiac sequelae.
After reviewing the English literature regarding treatment of DASS, we would like to emphasize some interesting points about the above-mentioned techniques:
Banding:
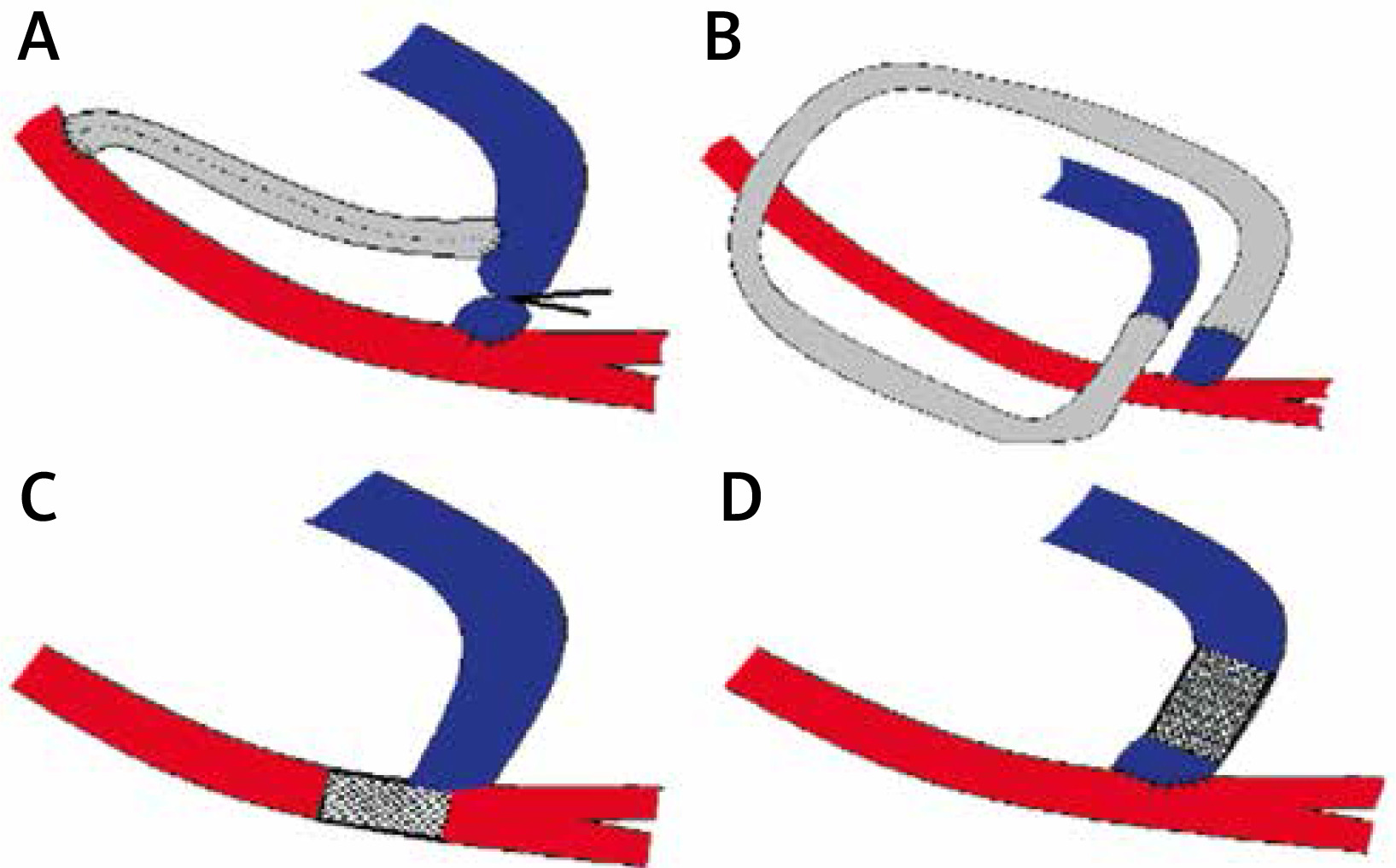
A prosthetic band (synthetic PTFE) 10-30 mm in length is wrapped around the outflow vein, near the anastomosis (Figure 1 A). In the past, the degree of banding was regulated intraoperatively by restoration of the radial pulse and preservation of thrill. Blind banding had poor results when no objective measure to determine the degree of stenosis was used [3]. It led to an unacceptably high rate of thrombosis (19%) and failure to treat symptoms (48%) [3]. But in our days, banding (BD) can be calibrated using intraoperative volume flow measurement with real-time CDU, measured 5 cm proximal to anastomosis [5–7]. Digital brachial pressure (DBP) > 50 mm Hg and DBI > 0.6 or waveform analysis has been used to prevent over-narrowing, intraoperatively [3]. Finger oximetry > 90%, restoration of radial pulse and relief of symptoms are further guiding parameters [6, 7]. Banding migration and proximal venous aneurysmal dilatation have been reported; thus band fixation is advocated [8]. The minimal accepted flow after banding to avoid AVA thrombosis is 400–600 for AVFs and 600–800 for grafts [5]. The post-stenotic turbulence was lower as the band was placed away from the anastomosis, about 2–3 cm [5]. A belt-shaped band has been reported that is of adjustable diameter according to flow until its final fixation [5].
Plication with metal clips or suturing along the outflow vein beyond the anastomosis over a Satinsky clamp (Figure 1 B). The best position of the clamp is decided according to intraoperative radial Doppler waveforms [3].
BD with a simple ligature (Figure 1 D). Some consider that multiple moderate stenoses from consecutive tight ligatures are preferable to a single ligature causing one severe stenosis [6, 7]. However, this approach lacks wide acceptance. Murray et al. demonstrated using a mathematical model that a 75% stenosis is required in an outflow vein 1 cm in diameter to reduce flow to 1000 ml/min [5]. The intended diameter after banding is at least 5 mm, which gives the optimal pressure of 40 mm Hg in the capillary bed. An increase in diameter by 1 mm increases the flow by 400 ml [5]. An interesting method is the MILLER (minimally invasive limited ligation endoluminal-assisted revision) banding procedure [7]. The tight ligature is placed over an intraluminal balloon usually sized 4 mm or 5 mm, 2–3 cm beyond the anastomosis, through 2 small skin incisions (Figure 2 A). Shukla et al. suggest a target banding diameter slightly smaller than the forearm artery with sluggish or reversed flow. Basically, they create a 75% lumen reduction to a mean diameter of 2.5 mm (2–3.5 mm). Some patients needed recurrent banding. Secondary patency was 59% at 1 year [7]. Others have used intraoperative CDU and pulse oximetry for a modified MILLER technique, reducing the diameter by 60–80% based on Murray’s nomogram [3, 6]. BD is calibrated with brachial artery flow measurement. If it is extreme, the vein is rebanded. If it is inadequate, angioplasty with a larger balloon is performed or the ligature is retied at a larger diameter [7]. Kok et al. advise a 75% reduction in diameter without flow monitoring. They recommend reducing under half the juxta-anastomotic vein diameter. They used a 5 mm balloon for a 13 mm vein and, interestingly, very small incisions [6]. The philosophy of the MILLER BD is preserved in the extraluminal banding technique, but it is simplified. A balloon or dilator (4, 5, or 6 mm) is placed extraluminally alongside the empty outflow vein (after clamping or using a pneumatic tourniquet) (Figure 2 B). After ligature placement the balloon or dilator is removed, and the vein lumen is expanded after release of perfusion at the predetermined diameter. The degree of BD is calibrated intraoperatively by pulse and thrill [7]. Dilators are preferred over balloons because they are not denting [6, 7]. A diameter between 3 and 4.5 mm is considered sufficient to treat most steals [5–7]. The primary patency was 100% at 1 year. Others used dowels with 0.5 mm increments to achieve the precise flow of 500–800 ml/min with two ties at the same site through a small skin incision [5–7].
Suture plication of the outflow vein (Figure 1 B). Staple aneurysmorrhaphy and BD with a 3.0 polypropylene tie over a 4 mm coronary dilator has been reported to treat Vascular access aneurysms (VAAs) (> 1.5 cm in diameter) and concomitant steal. Calibration with brachial flow measurement with CDU was apparent [3]. Simple BD in these cases would lead to steal recurrence due to remodeling of the folded vein wall [3].
Interposition of a 3–4 cm long and 4 mm in diameter graft has been reported (Figure 1 C) [9–11].
The RUDI technique includes fistula ligation and a short bypass (prosthetic or venous) between the outflow conduit and the proximal radial or ulnar artery (Figure 3 A) [3, 12]. A modification has been reported where, if there is enough room, the anastomosis is removed distally to the proximal radial or ulnar artery (secondary extension) (Figure 3 C) [12]. Translocation of the inflow site to the proximal forearm arteries leads to a > 50% reduction in access flow [12]. Additionally, it leaves undisturbed the alternate forearm artery to perfuse the arm via augmented flow [12]. RUDI has good patency rates (80–100%) and excellent symptom relief [3]. Secondary extension technique had a primary success of 96% and 10% fistula thrombosis at 12 months in one report [12]. If the proximal artery is enlarged, some prefer RUDI over BD as BD leads to steal recurrence [3]. A similar technique uses the radial artery, which is freed up and reversed in a loop fashion. Afterwards it is anastomosed to the cephalic vein and the AVF is ligated [13]. It is a technically demanding operation with satisfactory results (Figure 3 B) [13]. However, RUDI or secondary extension technique have been used in the literature despite volume flow [12, 14].
The DRIL procedure involves a preferably venous bypass originating at least 7 cm proximal to the brachial anastomosis and ending beyond it [3, 15]. The artery is ligated immediately distal to the brachial anastomosis (Figure 4 A). Reported technical success was 90% and at 4 years the bypass was patent in 80% of patients [4]. Some advocate against ligation because it increases the distal perfusion by only 10% (Figure 4 B) [15]. In this case the proximal anastomosis is constructed > 10 cm proximal to the brachial anastomosis [3]. The distal anastomosis can be constructed in end-to-end fashion (Figure 4 C). It is an effective procedure, but it needs general anesthesia, is technically demanding and has incision-related complications of 10–20% [15]. Moreover, limb perfusion is dependent on bypass patency and the limb’s viability is threatened; if there are bypass thromboses [3, 4]. PTFE grafts have a 43% thrombosis rate [14]. An arm vein conduit has fewer harvest site complications than saphenous vein harvesting and can be accomplished with local anesthesia [15]. However, use of an arm vein is controversial as it may be needed for future access. DRIL is indicated especially in low flow steal < 600 ml/min and works better in late onset steal [3].
PAI means to get arterial inflow from the axillary artery, which diminishes steal effects because of its larger diameter and higher pressures (Figure 5 A) [4]. After PAI the large collaterals of the proximal arteries are employed to aid in distal arm perfusion. Additionally, axillary branches could also be used for inflow, so that the axial axillary flow is not disturbed [3]. The disadvantage of PAI is the use of a prosthetic graft, which reduces the patency rates and increases the infection rates. In normal flow fistulas the first option is PAI and DRIL is reserved for fit patients with an adequate saphenous vein graft and healthy distal arteries [3].
Prolongation of existing grafts to treat steal syndrome increasing the outflow resistance has also been reported in high-flow AVAs [16, 17]. One technique reported included a loop synthetic tube graft 30 or 40 cm in length interposed in the divided cephalic vein near the brachiocephalic anastomosis [17]. It is placed in a loop fashion in the upper arm (Figure 5 B). A second technique reported the construction of a 5 mm forearm loop graft, 25 cm in length, after removal of a side-to-side brachiocephalic fistula [16]. The rationale behind all these procedures is that prolongation of the outflow bed increases resistance, diverting flow to the distal arterial conduit. Theoretically, prolongation is safer than anastomosis lessening or banding as small alterations in diameter give large alterations in flow volume [17].
In the case of a Brescia-Cimino fistula, distal radial artery ligation (DRAL) is suggested to halt retrograde flow from the palmar arch to the fistula (Figure 2 C) [1, 3]. Proximal ligation (PRAL) is suggested in high-flow AVF with cardiac complications and no arm ischemia (Figure 2 D).
Anastomosis reduction from within the outflow vein (anastoplasty). After a transverse vein incision close to the AVF, the anastomosis is partially sutured from inside (Figure 3 D) [18]. Percutaneously, a covered stent may be placed which partially protrudes in ¾ of the anastomosis area (Figure 5 C) [19]. Alternatively, a covered stent can be placed in the juxta-anastomotic outflow vein (Figure 5 D). Similarly, a tapered flared stent-graft can also be used in the same site to narrow the lumen as the flared portion is constrained by the diameter of the vein [20].
Ligation of the fistula is reserved for patients with limited life expectancy, a previous failed steal-correcting procedure, in ischemic monomelic neuropathy and in cases of gross ischemic lesions [1, 3].
Figure 1
A – Banding with a strip: a prosthetic PTFE-band is wrapped around the juxta-anastomotic outflow vein. B – Plication of the cephalic vein after careful adjustment of the Satinsky clamp position. C – Short interposition grafting 4 mm in diameter. D – Ligature banding

Figure 2
A – MILLER technique: a properly sized intravascular balloon determines the residual lumen after ligature banding, via a small incision. B – Balloon or dilator-assisted extraluminal banding technique: a properly sized extraluminal balloon determines the residual lumen after ligature banding, via a small incision. C – DRAL procedure. Distal radial artery ligation in Brescia-Cimino fistula. D – PRAL procedure. Proximal radial artery ligation in Brescia-Cimino fistula

Figure 3
A – The RUDI-1 technique: fistula ligation combined with a short bypass between the outflow conduit and the proximal radial or ulnar artery. B – The RUDI-2: Translocation of the radial artery which supplies the AVF after ligation. C – The RUDI-3: the anastomosis is removed distally to the proximal radial or ulnar artery. D – Anastoplasty: the anastomosis is partially sutured from inside

Figure 4
A – The DRIL procedure: a preferably venous bypass is constructed to supply the distal arm after ligation of the brachial artery just distal to the AVF. B – The DRIL without arterial ligation. C – The distal anastomosis may be constructed in end-to-end fashion

Figure 5
A – The PAI procedure. Arterial inflow is taken from the larger diameter axillary artery. B – Prolongation of an existing AVF/AVG increases the outflow resistance. A loop synthetic tube graft is interposed in the divided cephalic vein. C – The covered stent partially protrudes in the anastomosis. D – The covered stent narrows the juxta-anastomotic outflow vein lumen