

Purpose
With recent advances in breast cancer loco-regional and systemic therapies, which resulted in high survival rates, cosmetic outcomes became more important [1, 2]. In addition, better recognition of risk factors contributing to poor cosmetic results may improve the quality of life of these patients [2].
Breast conservation surgery (BCS) plus whole breast irradiation (WBI) is the standard of care in early-stage breast cancer [3]. Also, there is evidence that a tumor bed boost enhances local control, especially in young patients, and in the presence of lympho-vascular space invasion or positive or close surgical margins [4, 5].
Low-energy electrons (range, 9-12 MeV) are widely used for delivering the boost dose. However, considering their limited therapeutic range, only superficial regions of the breast can be effectively irradiated. Using higher energy electrons to treat deeper areas of the breast results in overdosing of skin, normal breast, lungs, and heart, and also may have a negative impact on breast cosmesis. In this context, the EORTC boost trial showed that high energy electrons were linked to a higher 10-year risk of severe breast fibrosis.
Other techniques for tumor bed boosting, especially deep-seated tumor beds, are external beam radiation therapy (EBRT) and multicatheter interstitial brachytherapy (MIBT). Data regarding the pros and cons of these boost techniques in terms of effectiveness, toxicity, and cosmetic results are limited, and the most published data on MIBT boost comes from time before the widespread availability of high-dose-rate (HDR) sources, computerized remote after loaders, stepping source technology, cross-sectional image-based treatment planning, and inverse optimization algorithms. The advantage of each boost modality depends on breast anatomy and lumpectomy cavity location. For a shallow target, if the breast contour is roughly flat and beam obliquity can be avoided, en-face low energy electron beam is the preferred technique, as electron beam obliquity reduces its’ therapeutic range and increases the skin absorbed dose [6]. In deep-seated tumor beds (depth ≥ 4 cm), modern image-guided multicatheter interstitial brachytherapy boost in comparison with other boost modalities, such as high energy electron beams or advanced external beam photon techniques (e.g., intensity modulated radiation therapy [IMRT] or volumetric modulated arc therapy [VMAT]), can better protect nearby healthy organs from high doses of radiation, and therefore are an excellent modality for dose escalation [6-8].
In electron and external beam photon boosts, even if accompanied by modern treatment verification techniques, a larger volume (compared to brachytherapy) need to be irradiated to account for inter- and intra-fractional organ motions, and accelerator and patient’s setup uncertainties (planning target volume concept). These problems are irrelevant for MIBT. Multicatheter interstitial brachytherapy, as a minimally invasive procedure, has its’ limitations, including relative patient discomfort and the necessity of significant learning curve [6].
Several patient, tumor, and treatment-related factors have been connected to sub-optimal cosmetic outcomes after breast conservation therapy, but the results are not consistent across studies (many of them lack objective assessment of breast cosmesis). These factors include high body mass index (BMI), age (both younger and older patients), breast volume, inner quadrant tumor location, tumor size, extent of breast surgery (volume of tissue removed from the breast at lumpectomy), type of surgical incision, complete axillary dissection (versus sentinel node biopsy), receiving chemotherapy, regional nodal irradiation, higher total radiation doses (to the breast’s skin and tissue), conventionally fractionated regimens (versus hypofractionated schedules), receiving a boost, boost technique, and higher boost volumes [2, 9-13]. Additionally, in patients treated with an interstitial brachytherapy boost, the number of implanted catheters and automatic optimization technique (vs. manual optimization) have been reported to be inversely correlated with breast cosmesis [10].
This study was designed to measure breast cosmesis in breast cancer patients treated with adjuvant WBI plus high-dose-rate MIBT boost after BCS, both objectively by BCCT.core software (using front view digital photographs) and subjectively with Harvard’s score. Also, to identify patient, tumor, and treatment factors, including dosimetric parameters of external beam and brachytherapy plans, which predict poor cosmetic scores.
Material and methods
Study design
In this retrospective research, cosmetic outcomes of 28 consecutive breast cancer patients treated with adjuvant WBI plus HDR-MIBT boost after BCS (± adjuvant chemotherapy and/or hormone therapy) at Radiation Oncology Department of Ahvaz Golestan Hospital (Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran) between 2017-2018 were objectively measured with BCCT.core software using a front view digital photograph, and subjectively evaluated according to Harvard’s scale. Informed consent for taking photographs and reviewing medical records was obtained from every participant included in the study. In our center, HDR interstitial brachytherapy boost are offered to patients at higher risk for local recurrence (e.g., young age, LVSI, and close or positive surgical margins) or with deep-seated tumor beds unsuitable for low energy electron boosts. Single cross-sectional cosmetic scoring was performed at least 12 months after completion of radiation therapy treatments. Moreover, to evaluate the correlation between cosmetic outcomes and dose-volume histogram (DVH) parameters, external beam and brachytherapy treatment plans were retrospectively analyzed, and ipsilateral skin and breast tissue dosimetric indices were recorded.
Whole breast irradiation
All patients received a total dose of either 50 Gy in 25 fractions, 50.4 Gy in 28 fractions, or 42.5 Gy in 16 fractions using opposed tangential photon beams (± irradiation of regional lymphatics at the discretion of treating physician). A collapsed cone super-position algorithm was applied for EBRT dose calculations (Isogray v. 4.2.265L, Dosisoft, Cachan, France).
HDR interstitial brachytherapy boost
Boost dose (13.6 Gy in 4 bid fractions) was delivered at 1 to 2 weeks either before or after WBI using a 60Co source. In all patients, catheter implantation, contouring, and dose calculations (based on TG-43 formalism) (HDR Plus v. 3.0.7.0, Eckert & Ziegler BEBIG GmbH, Germany) were performed with adherence to GEC-ESTRO guidelines [14].
Cosmesis evaluation
BCCT.core software: For this purpose, front view digital photographs were obtained from enrolled patients (in arm down position) and imported to the software. All photographs were captured in the same room under the same light conditions, and also with the same camera and photographer. After marking the nipples, breasts contours, and sternal notch on the patient’s photograph and adjusting the image scale, the software automatically classified the patient’s aesthetics into four categories, including excellent, good, fair, and poor based on asymmetry, color, and scar measures [15].
Harvard’s scale: Aesthetic results were subjectively classified by a physician (NF) into four groups, such as excellent (if the treated breast was nearly identical to the untreated one), good (if the treated breast was slightly different from the untreated breast), fair (if the treated breast was clearly different from the untreated breast, but not seriously distorted), and poor (if the treated breast was seriously distorted) [16].
Contouring
Ipsilateral breast: This organ was contoured according to the ESTRO guidelines [17]. It should be noted that in brachytherapy treatment plans, clinical target volume (CTV) was included in this volume.
Ipsilateral skin: This structure was defined as a 5 mm layer underneath the skin surface on the involved breast [14].
Biologically effective dose-volume histogram parameters (α/β = 3 Gy)
Table 1 presents ipsilateral skin and breast histogram parameters (from external beam whole breast and brachytherapy boost treatment plans) that we reported in this study. Due to our technical limitation, since separate software was used for external beam and brachytherapy treatment plannings, cumulative (WBI + MIBT) DVH parameters could not be calculated.
Table 1
Histogram parameters reported and analyzed in this study
Statistical analysis
Jamovi software version 1.6.23.0 was applied for statistical analysis [18]. Medians (with 25-75th percentiles) were reported to describe the central tendency of data. The correlation between variables was assessed with Spearman’s rank test. Univariate ordinal logistic regression analysis was conducted to screen for significant predictors of breast cosmesis scores. For each variable, p-value, odds ratio, and 95% confidence interval were calculated. Then, variables with a p-value < 0.1 obtained from univariate analysis were entered into a multivariate ordinal logistic regression model. P-value < 0.05 in the final model was considered statistically significant.
Results
Patient, tumor, and treatment characteristics are summarized in Table 2. The median time from completion of radiation therapy to cosmesis scoring was 18 months. In cosmesis evaluation with BCCT.core software, no patient was scored as excellent. Cosmesis was good in 5 (18%), fair in 14 (50%), and poor in 9 (32%) patients. According to the Harvard’s scale, 3 (10.5%) patients had excellent cosmesis. Moreover, 12 (43%), 8 (28.5%), and 5 (18%) patients had good, fair, and poor Harvard’s scores, respectively (Figure 1). There was a statistically significant strong direct correlation between BCCT.core and Harvard’s scores (p = 0.002) (Spearman’s coefficient = 0.54) (Figure 2).
Table 2
Patient, tumor, and treatment characteristics
a Median (25-75th percentile); bfinal lumpectomy specimen volume + excisional biopsy specimen volume; cAC: doxorubicin + cyclophosphamide; dT: paclitaxel; eEC: epirubicin + cyclophosphamide; fTCH: docetaxel + carboplatin + trastuzumab; gat the time of cosmesis evaluation; WBI – whole breast irradiation; MIBT – multicatheter interstitial brachytherapy; GnRH – gonadotropin-releasing hormone
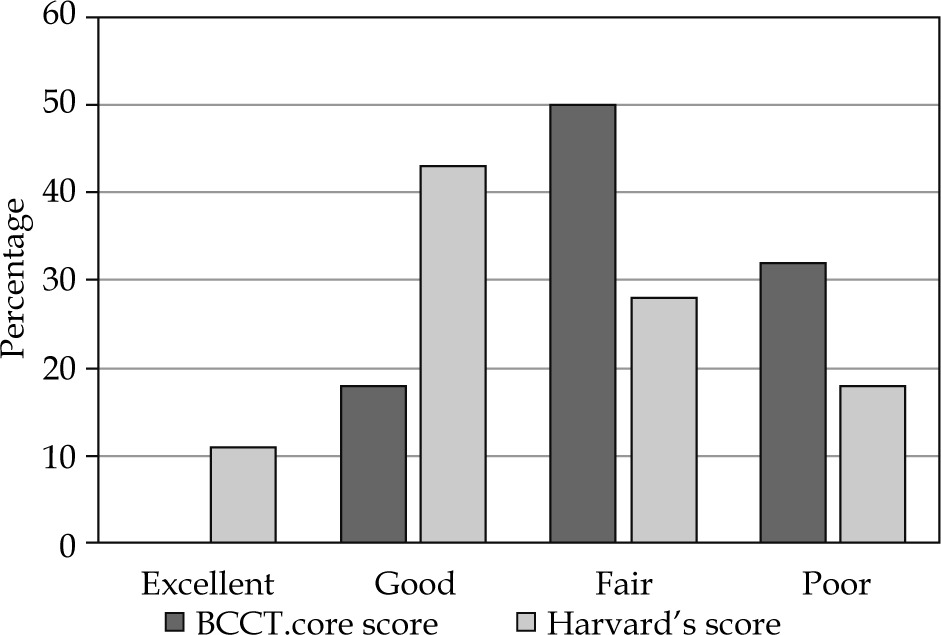
Fig. 2
This scatter plot illustrates the strong positive correlation between BCCT.core and Harvard’s scores

Absolute values of ipsilateral breast and skin biologically effective V parameters in WBI and MIBT plans are summarized in Table 3. WBI and MIBT relative dose-volume histograms are shown in Figures 3 and 4. In WBI, the median breast and skin biologically effective maximum doses (BEDmax) (25-75th percentile) were 114 Gy (range, 109-118 Gy) and 108 Gy (range, 104-113 Gy), respectively. Skin D parameters in MIBT plans are presented in Table 4.
Fig. 3
Whole breast irradiation relative ipsilateral breast and skin biologically effective dose-volume histogram

Fig. 4
Multicatheter interstitial brachytherapy relative ipsilateral breast and skin biologically effective dose-volume histogram

Table 3
Absolute ipsilateral breast and skin biologically effective V parameters
Table 4
Numerical values of skin D parameters for brachytherapy boost (ipsilateral side)
| Parametera | Median (25-75th percentile) (Gy) |
|---|---|
| D0.01cc | 302 (21-838) |
| D0.1cc | 120 (19-234) |
| D0.2cc | 79 (18-140) |
| D0.5cc | 48 (17-87) |
| D1cc | 39 (16-62) |
| D2cc | 33 (13-44) |
| D5cc | 22 (9-29) |
In univariate analysis, no patient (age, follow-up time, breast volume, and breast tumor location), tumor (pT stage, pN status, and tumor size), and treatment characteristics (lumpectomy specimen volume, hormone therapy regimen, WBI dose-fractionation schedule, before or after EBRT brachytherapy boost timing, and regional nodal irradiation), or dosimetric parameters were predictive of BCCT.core scores. Only there was a trend for higher BCCT.core scores in pN-positive cases, and patients who received regional nodal irradiation. In contrast, receiving regional nodal irradiation (p = 0.039), larger breast volumes (p = 0.037), higher WBI absolute breast V86Gy (p = 0.038), and higher MIBT absolute breast V29Gy (p = 0.037) were significant predictors of poorer Harvard’s scores. Also, there was a trend for higher Harvard’s scores in pN-positive cases, patients with higher WBI absolute breast V90Gy, and higher MIBT absolute breast V36Gy, V43Gy, V50Gy, and V57Gy (Table 5).
Table 5
Ordinal logistic regression analysis
On multivariate analysis, none of the demographic factors, tumor, and treatment characteristics, or dose-volume histogram parameters remained statistically significant for predicting Harvard’s score. Only there was a trend for higher Harvard’s score in patients with higher MIBT absolute breast V29Gy (p = 0.066) (Table 5).
Discussion
In recent two decades, the widespread availability of electron beams combined with their relative comfort of use, has led to decreased use of interstitial brachytherapy for delivering boost dose. In fact, in superficial lumpectomy beds, if the breast contour is roughly flat and beam obliquity could be avoided, the preferred modality for breast boost is low energy electrons. However, in women with large breasts and centrally located deep-seated tumor bed, MIBT boost could be a great tool in radiation oncology armamentarium, since it can better protect nearby tissues from high doses of radiation in comparison with high energy electrons (> 12 MeV) due to increased skin dose, or sophisticated photon EBRT techniques. Additionally, with a MIBT boost, safer dose escalation is achievable in patients with a higher risk for local recurrence [6].
Recently, following the availability of highly effective systemic treatments for breast cancer, and as a consequence of longer survivals in these patients, long-term treatment toxicity and cosmetic outcomes have become more important. Therefore, the present study assessed the potential patient, tumor, and treatment-related factors, which could predict poor cosmesis in patients treated with WBI + MIBT boost [1,2].
In our study, 18% and 53.5% of patients had an excellent or good cosmesis according to BCCT.core and Harvard’s scores, respectively. Since baseline (pre-RT) cosmesis scoring was not performed, relative effects of surgery, chemotherapy, and radiation on cosmesis could not be distinguished. The Harvard score results are compatible with Polgár et al. [19] retrospective study showing 56% of excellent or good cosmesis, and contradictory to Rulli et al. [20] and Dolezel et al. [21] prospective studies, with 97% and 82.6% of excellent or good cosmesis, respectively. In our literature review, no study that used the BCCT.core objective scoring system for cosmesis evaluation was found (Table 6).
Table 6
Summary of the cosmetic outcomes after high-dose-rate (HDR) brachytherapy boost from the available studies
| Authors, publication year, [Ref.] | Study type | Patient accrual date | Patient No. | Median patient age (years) | Catheter implantation timing | Dose fractionation regimen | Median follow-up (months) | Cosmesis evaluation method | Cosmetic outcome | Predictors of cosmesis | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| EBRT | BRT boost | Excellent | Good | Excellent + good | |||||||||
| Manning et al. (2000) [9] | Pros. | 1994-1996 | 18 | 53 | Post-op | 50-50.4 Gy | 15 Gy/6 fx. | 50 | N/R | 22% | 45% | 67% | Excision volume |
| Berberich et al. (2001) [25] | Pros. | 1986-1997 | 100 | 52 ±11a | Intra-op | 42 Gy (range, 36-50)b | 18 Gy | 113 | N/Rc | 28% | 39% | 67% | – Total dose to remaining glandular tissue – Boost dose |
| Polgar et al. (2002) [26] | Pros. | 1995-1998 | 52 | 52 | Post-op | 50 Gy/25 fx. | 12-14.25 Gy/ 3 fx. | 64 | Perez et al. scale | N/R | N/R | 88.5% | – |
| Tortajada et al. (2005) [27]d | Pros. | 1999-2000 | 84 | N/R | Post-op | 46 Gy | 7 Gy | 43 | N/R | N/R | N/R | 95% | – |
| Budrukkar et al. (2007) [11] | Retro. | 1980-2000 | 145 | 45 | Post-op | 45 Gy/25 fx. | 10 Gy/1 fx. | 36 | JCRT scale | N/R | N/R | 83.5% | Adjuvant chemotherapy |
| Guinot et al. (2007) [28] | Pros. | 1996-2000 | 125 | 55 | Post-op | 50 Gy | 13.2 Gy/3 fx. | 84 | N/R | N/R | N/R | 77% | – |
| Kulik et al. (2009) [10] | Pros. | 1996-1999 | 93 | 50.8a | Post-op | 50 Gy/25 fx. 50 Gy/20 fx. | 10 Gy/1 fx. | 55.4 | Modified EORTC scale | 41%e (54%f) | 44%e (28%f) | 85%e (82%f) | – Clinical and mammographic tumor estimation – Method of breast conserving surgery – Type of skin incision – Number of interstitial catheters – Irradiated reference volume (PTV) – Optimization method |
| Rulli et al. (2010) [20] | Pros. | 2003-2007 | 5 | 65 | Intra/Post-op | N/R | 9 Gy/1 fx. 12 Gy/3 fx. | 32 | Harvard’s criteria | 74% | 23% | 97% | – |
| Polgár et al. (2010) [19] | Retro. | 1995-2007 | 79 | 56.7 | Post-op | 50 Gy (30-50) | 10.35 Gy/1 fx. 12.8 Gy/2 fx. 14.25 Gy/3 fx. | 90 | Harvard’s criteria | 17% | 39% | 56% | – High boost dose (20 Gy LDR equivalent) – High DNR value |
| Perez et al. (2012) [29] | Pros. | 1996-2005 | 63 | N/R | Post-op | 50 Gy/25 fx. | 7 Gy | 36 | Fehlauer’s scalee Five-level scalef | N/R | N/R | 84.8e (96.5%f) | – Extensive surgery – High T stage – Implant volume |
| Dolezel et al. (2012) [21] | Pros. | N/R | 23 | 46 | Intra-op | 48.6 Gy/27 fx. | 12 Gy/4 fx. | 43.3 | Harvard’s criteria | N/R | N/R | 82.6% | – Starting irradiation immediately after or too soon after surgery – Using a single-large HDR dose – Method of planning (3D CT-based HDR-BRT with optimization) – Neoadjuvant chemotherapy |
| Roy et al. (2013) [30] | Pros. | 2005-2007 | 20 | N/R | Post-op | 50 Gy/25 fx. | 15 Gy/3 fx. | N/R | CTCAE (ver. 2) | 50% | 30% | 80% | – |
| Sharma et al. (2013) [31]d | Pros. | 2005-2010 | 100 | 46 | Peri-op | 50 Gy | 15 Gy/6 fx. | 52 | N/R | N/R | N/R | 87% | – |
| Guinot et al. (2015) [32] | Pros. | 1999-2007 | 167 | 41 | Post-op | 46-50 Gy | 7 Gy | 92 | N/R | N/R | N/R | 97% | – |
| Cambeiro et al. (2016) [22] | Pros. | 2004-2014 | 34 | 62 | Intra-op | 39.9 Gy/15 fx. | 13.6 Gy/4 fx. | 8.7h | Wazer’s criteria | 11.7% | 64.7% | 76.4% | – Minimal breast implantg – Small CTV volumeg – Exigent skin dose constraintsg |
| Quéro et al. (2017) [23] | Retro. | 1990-2002 | 264 | 56.7 | Intra/Post-op | 44 Gy/20 fx. | 10 Gy/2 fx. | 124 | RTOG/EORTC LENT-SOMA | N/R | N/R | 80% | – Small boost volume (mean V100: 45.8cc)g – Implantation of 3 catheters in a single-planeg |
| Matuschek et al. (2019) [33] | Retro. | 1991-1999 | 43 | 53 | Post-op | 50 Gy/25 fx. | ≥ 10 Gy | 17.7 | Harvard’s criteria, Cocquyt’s score BRA score | 80% | 50% | 30% | – |
| Morales et al. (2020) [24] | Pros. | 2008-2016 | 12 | 52 | Intra-op | 39.9 Gy/15 fx. | 13.6 Gy/4 fx. | 89 | Wazer’s criteria | 33.3% | 33.3% | 67% | – V100 > 10% – Higher BED |
| The current study results | Retro. | 2017-2018 | 28 | 48 | Post-op | 50 Gy/25 fx. 50.4 Gy/28 fx. 42.5 Gy/16 fx. | 13.6 Gy/4 fx. | 18 | BCCT.core, Harvard’s criteria | 0%i, 10.5%j | 18%i, 43%j | 18%i, 53.5j | – Absolute breast V29Gyk,l – Positive axillary lymph nodes and regional nodal irradiationk – Breast volumek |
a Mean ± standard deviation; b2.4 Gy/fx.; csymmetry assessed; donly abstract reviewed; eevaluation by physicians; fevaluation by patients; gfactors related to good cosmetics; hminimum; iBCCT.core; jHarvard’s criteria; kbased on trends (not statistically significant in multivariate analysis); lvolume of the breast in centimeter cube that received 29 Gy biologic effective dose (α/β = 3 Gy for normal breast late effects) BED – biologically effective dose; BRA – breast retraction assessment; BRT – brachytherapy; CTCAE – common terminology criteria for adverse events; CTV – clinical target volume; DNR – dose non-uniformity ratio; EBRT – external beam radiation therapy; EORTC – European Organization for Research and Treatment of Cancer; HDR – high-dose-rate; Intra-op – intra-operative; JCRT – Joint Centre for Radiation Therapy; LENT-SOMA – late effects normal tissue task force-subjective, objective, management, and analytic; LDR – low-dose-rate; N/R – not reported; Peri-op – perioperative; Post-op – post-operative; Pros – prospective; PTV – planning target volume; RTOG – Radiation Therapy Oncology Group
In the multivariate model, we did not find any statistically significant patient, tumor, or treatment-related factor for cosmesis prediction. There was a trend for poorer cosmesis in patients with higher absolute, but not relative, MIBT V29Gy (volume of the breast tissue that received 100% of the prescribed dose in brachytherapy boost, if α/β = 3 Gy was assumed for normal breast late effects), with odds ratio = 1.01, meaning that every centimeter cube increase in MIBT breast V100% (treated volume) increases the risk of poorer Harvard’s score by 1%. This finding is in line with Kulik et al. [10], Cambeiro et al. [22], Quéro et al. [23], and Morales et al. [24] studies (Table 6). In univariate analysis, patients treated with irradiation of regional lymphatics (odds ratio ≈ 5), and patients with larger breast volumes presented statistically significant poorer cosmesis scores. Wang et al. [2], in a prospective longitudinal study, found that larger breast volumes and supra-clavicular regional nodal irradiation are associated with worse breast asymmetry one year after EBRT. Larger breast volumes or using a supra-clavicular field is often accompanied by a heterogeneous dose distribution (more hot spots) in EBRT planning. Other proposed mechanisms are higher susceptibility of breast adipose tissue to radiation-induced atrophy and radiation damage to regional lymphatics [2].
The small sample size and short follow-up times are the main limitations of the current study that preclude reaching a statistical significance. Moreover, due to the retrospective nature of this study, baseline (pre-RT) cosmetic scores were not available, therefore the impact of surgery or chemotherapy on cosmesis could not be distinguished from radiation therapy. Another problem was that since different software was used for EBRT and brachytherapy plannings, cumulative DVH parameters (WBI + MIBT) could not be calculated.
One strength of our study was that biological equivalent dose-volume parameters were used instead of physical ones to eliminate the impact of dose-fractionation regimens used for WBI and MIBT; thus, the study results can become more generalizable. Also, observer-independent objective measures (BCCT.core) for cosmesis scoring in addition to traditional subjective methods (Harvard’s method) were applied.
Conclusions
Based on the findings of our study, higher absolute breast V29Gy in multicatheter interstitial brachytherapy boost, regional nodal irradiation, and large breast volumes are the potential candidates that could have deleterious effects on cosmesis in breast cancer patients treated with whole breast radiotherapy plus HDR interstitial brachytherapy boost after breast conservation surgery. Larger-scale longitudinal prospective studies with longer follow-up durations are needed to confirm these results.